Biomed Res Bull. 2(2):87-95.
doi: 10.34172/biomedrb.2024.14
Review Article
The Effectiveness of Kinesio Taping in Pregnancy-Related Back and Pelvic Girdle Pain: A Systematic Review and Meta-Analysis
Kimia Motlagh Asghari 1  , Vahideh Toopchizadeh 1, Yasaman Mirzazadeh 2, Fereshteh Jamali 3, Neda Dolatkhah 1, *
, Vahideh Toopchizadeh 1, Yasaman Mirzazadeh 2, Fereshteh Jamali 3, Neda Dolatkhah 1, *
Author information:
1Physical Medicine and Rehabilitation Research Center, Tabriz University of Medical Sciencse, Tabriz, Iran
2Faculty of Medicine, Ardabil University of Medical Sciences, Ardabil, Iran
3Immuonology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background:
Using Kinesio tape (KT) in managing low back pain among pregnant and postpartum women has gained significant attention. This systematic review and meta-analysis aimed to evaluate the effectiveness of KT interventions in reducing pain intensity and disability levels in this population.
Methods:
A systematic search was conducted in English-language databases, including PubMed, EMBASE, Web of Science, ClinicalTrials.gov, Scopus, PEDro, AMED, and Iran Medex, with no time restrictions up until April 2024.
Results:
Ten randomized controlled trials (RCTs) met the inclusion criteria, investigating the effects of KT in pregnant and postpartum women with back and pelvic girdle pain. The risk of bias was assessed using the Cochrane risk of bias tool. The results indicated a significant improvement in pain intensity and disability among participants who received KT interventions.
Conclusion:
Despite variations in study design and sample sizes, the overall findings suggest a positive effect of KT in reducing back and pelvic girdle pain during pregnancy and the postpartum period. However, further research with larger sample sizes and more robust study designs is necessary to confirm these findings.
Keywords: Pregnancy, Physical therapy method, Back pain, Pelvic girdle, Conventional treatment methods, Kinesio tape
Copyright and License Information
© 2024 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This study was self-funded by the authors and received no external financial support from any funding organization.
Introduction
Pregnancy is a unique physiological condition characterized by various musculoskeletal changes, including alterations in posture and weight distribution, which often lead to discomfort and pain, particularly in the back and pelvic girdle regions.1 Pregnancy-related back pain and pelvic girdle pain are common complaints among expectant mothers, affecting up to 50%-70% of pregnant women at some point during their gestation.2 Back pain during pregnancy typically presents as discomfort localized in the lumbar vertebrae, often extending to the legs, and is exacerbated by prolonged periods of sitting, standing, or lifting objects.3,4 Additionally, pregnant women may experience heightened sensitivity in the paraspinal muscles upon palpation.5 Conversely, pelvic girdle pain manifests by discomfort in the lower lumbar and sacral regions, particularly around the sacroiliac joints.6 This pain may radiate to the hips and thighs, significantly impairing mobility and daily activities. The onset of back pain generally occurs around the 22nd week of pregnancy7 and affects more than half of all pregnant women.8 These conditions not only reduce the quality of life for expectant mothers but can also hinder their ability to perform daily activities, potentially contributing to negative pregnancy outcomes such as preterm birth, low birth weight, or complications for the newborn. In severe cases, these conditions may also increase the risk of miscarriage or stillbirth.9,10 Although pregnancy-related back and pelvic girdle pain are not life-threatening, they impose considerable physical, emotional, and social burdens on affected individuals.11 Persistent pain and disability, coupled with associated challenges such as sexual dysfunction, reduced work capacity, and heightened psychological stress, can severely disrupt maternal well-being and daily functioning during pregnancy and the postpartum period.12,13
Considering the adverse effects of pregnancy-related back and pelvic girdle pain, there is an urgent need for actual management approaches tailored to this population.1,9 Conservative approaches are often preferred to avoid pharmacological interventions during pregnancy, highlighting the importance of non-invasive, low-risk treatment strategies.5 In recent years, there has been increasing interest in non-pharmacological interventions to address pregnancy-related back pain and pelvic girdle pain, due to the limitations and possible risks associated with pharmacotherapy during pregnancy.
Although several conservative interventions such as manual therapy, ergonomic adjustments, massage, and electrotherapy have been suggested, consensus regarding their optimal application and timing remains unclear.5,6 The effectiveness of various conservative interventions and physical therapy modalities in managing pregnancy-related back and pelvic girdle pain has been the focus of research. Among these interventions, Kinesio tape (KT) has developed as a promising modality for managing musculoskeletal pain and dysfunction due to its non-invasive nature and potential to provide both support and pain relief without medication. KT involves the application of elastic therapeutic tape to the skin, which is thought to promote physiological movement and support affected muscles and joints.14 Although pregnant women may face challenges in independently applying KT due to changes in body shape, the involvement of a healthcare professional can help ensure proper application and maximize its benefits. Despite the growing popularity of KT in clinical practice, evidence concerning its effectiveness in managing pregnancy-related back pain and pelvic girdle pain remains inconclusive. Previous systematic reviews and meta-analyses have attempted to evaluate the efficacy of non-pharmacological interventions, including KT, but methodological discrepancies and limitations have hindered definitive conclusions.7,8
Furthermore, the methodological quality and heterogeneity of existing research pose challenges in drawing conclusive inferences regarding the efficacy of KT in this population. While some investigations have reported positive consequences, others have failed to establish significant benefits over conventional treatments or placebo interventions.15
Given the ongoing need for comprehensive and methodologically rigorous assessments, this systematic review aimed to critically evaluate the effectiveness of KT specifically in managing pregnancy-related back and pelvic girdle pain. To address these gaps, we conducted a systematic review and meta-analysis using a well-defined PICOT framework:
-
Population (P): Pregnant and postpartum women experiencing low back pain and/or pelvic girdle pain, excluding those with specific pathological conditions (e.g., fractures or severe systemic conditions).
-
Intervention (I): Application of KT, aimed at reducing pain and improving functional capacity.
-
Comparator (C): Comparison with placebo tape, standard pregnancy care, exercise programs, or no intervention.
-
Outcome (O): Primary outcomes include pain intensity and functional disability
-
Time (T): The duration of interventions ranged from one day to five weeks, capturing both short-term and mid-term effects.
This review sought to provide a robust analysis of the existing literature, addressing gaps and limitations identified in previous studies. Through a meticulous examination of the available evidence, this systematic review aimed to offer insights into the potential role of KT as a viable therapeutic option in the management of pregnancy-related musculoskeletal pain. By elucidating the effectiveness of KT and its implications for clinical practice, this review endeavored to contribute to the optimization of care for pregnant women experiencing back and pelvic girdle pain, ultimately enhancing their quality of life during pregnancy and postpartum recovery.
Methods
This systematic review was conducted in accordance with the guidelines set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).16
Literature Search
A comprehensive literature search was conducted on April 1, 2024, with no time restrictions, across multiple databases such as PubMed, EMBASE, Web of Science, ClinicalTrials.gov, Scopus, PEDro, AMED, and Iran Medex. The Google Scholar search engine was also used to increase the number of retrieved papers in English.
The search strategy was according to the PICO system. Medical Subject Headings (MeSH) were applied to identify keywords. English keywords derived from MeSH headings included (“pregnancy” OR “pregnant women” OR “perinatal care” OR “postnatal care”) AND (“Pelvic Girdle Pain” OR “low back pain” OR “Lower Back Pain” OR “Low Back Ache” OR “Low Backache”) AND (“Kinesio tape”). Moreover, the reference lists of eligible papers were reviewed to identify additional relevant studies.
In addition, to identify any further eligible studies, we manually screened the first 300 hits from the Google Scholar search engine. We also conducted backward and forward citation searches for all included studies. A detailed breakdown in the various stages of the search strategy for each database is presented in Table S1 (see Supplementary file 1).
Study Selection
The studies identified through electronic and manual searches were all imported into EndNote 20 (Clarivate Analytics, USA). After removing duplicate records, two authors (Y.M. and K.M.A.) independently screened the titles and abstracts of all studies based on the inclusion and exclusion criteria. Following the preliminary screening, irrelevant studies were excluded, and the same two authors thoroughly examined the full texts of the retained studies based on the prearranged inclusion and exclusion criteria. Any discrepancies between the reviewers were resolved by consulting a third author (N.D.). Additionally, two independent reviewers (K.M.A. and F.J.) screened the titles, abstracts, and full texts of potentially eligible studies.
The PICOT (Population, Intervention/Exposure, Comparison, Outcomes, and Time) framework was used to express the study question as follows:
-
Population: Pregnant women or women in the postpartum period experiencing back pain or pelvic girdle pain that is not attributed to a specific medical condition(e.g., diagnosed spinal disorder, herniated discs, fractures, or other structural or neurological abnormalities identified by a medical doctor).
-
Intervention/Exposure: Application of KT.
-
Comparison: Usual/standard care for pregnancy-related back pain or pelvic girdle pain, without exposure to the KT (not necessary);
-
Outcomes: Primary outcomes included a reduction in pain intensity measured using visual analog scales (VAS), numerical pain rating scales (NPRS), brief pain inventories (BPI), and McGill pain questionnaires (MPQ). Secondary outcomes included reductions in disability as measured by the Oswestry Back Pain Disability Inventory (ODI), Quebec Back Pain Disability Scale (QBPDS), Roland Morris Disability Questionnaire (RMDQ), and Back Pain Function Scale (BPFS).
-
Time: Time is defined as post-intervention outcomes, measured at various follow-up points (ranging from 1 day to 5 weeks, depending on the study).
Studies were included if they met the following criteria: (1) randomized or quasi-randomized clinical trials, (2) involving pregnant or postpartum women with back pain or pelvic girdle pain, (3) evaluating the effectiveness of KT as an intervention, (4) reporting outcomes related to pain intensity and/or disability, and (5) published in English. Studies were excluded if they did not focus on KT as the intervention, involved participants with specific medical conditions affecting the spine (e.g., diagnosed spinal disorder, herniated disc, and fracture), or were not published in English.
Data Extraction
Data extraction was performed using a standardized form to capture study characteristics, participant demographics, intervention details, outcome measures, and results. Two reviewers independently carried out the data extraction process using predefined forms. The extracted data from each included study encompassed the following aspects: (1) study details, including the first author’s name, title, country, publication year, and study design, (2) study population and sample size, (3) details of the methods used, (4) outcome measures.
Critical Appraisal
Two reviewers independently evaluated the risk of bias and study eligibility using the Cochrane Collaboration’s Risk of Bias (RoB).17 This tool assesses the risk of bias across several domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Each domain is categorized as having a low, high, or unclear risk of bias. For example, in the domain of random sequence generation, a low risk of bias indicates that the sequence generation process was adequately described and was unlikely to lead to systematic differences between intervention groups. In contrast, a high risk of bias suggests that the sequence generation process was inadequate or not reported, increasing the likelihood of systematic differences between groups. An unclear risk of bias indicates insufficient information to make a judgment.
Data Synthesis
Meta-analysis was conducted using RevMan software (Version 5.4, Cochrane Collaboration). Continuous outcomes were analyzed using mean differences (MD) with 95% confidence intervals (CI). Cochran’s Q test and Higgins I2 statistics were employed to evaluate the heterogeneity of studies. Sensitivity analysis was conducted by removing individual studies one by one to evaluate the robustness of the results. Funnel plots were used to evaluate publication bias. All P values were two-tailed, and a P value < 0.05 was considered statistically significant.
Results
Search Results and Study Selection
The systematic search identified a total of 1483 potentially relevant articles and reports. After removing duplicates and screening titles and abstracts, 63 full-text articles were assessed for eligibility. Of these, 7 randomized clinical trials18-24 and 3 quasi-experimental studies25-27 met the inclusion criteria and were included in the review (Figure 1).
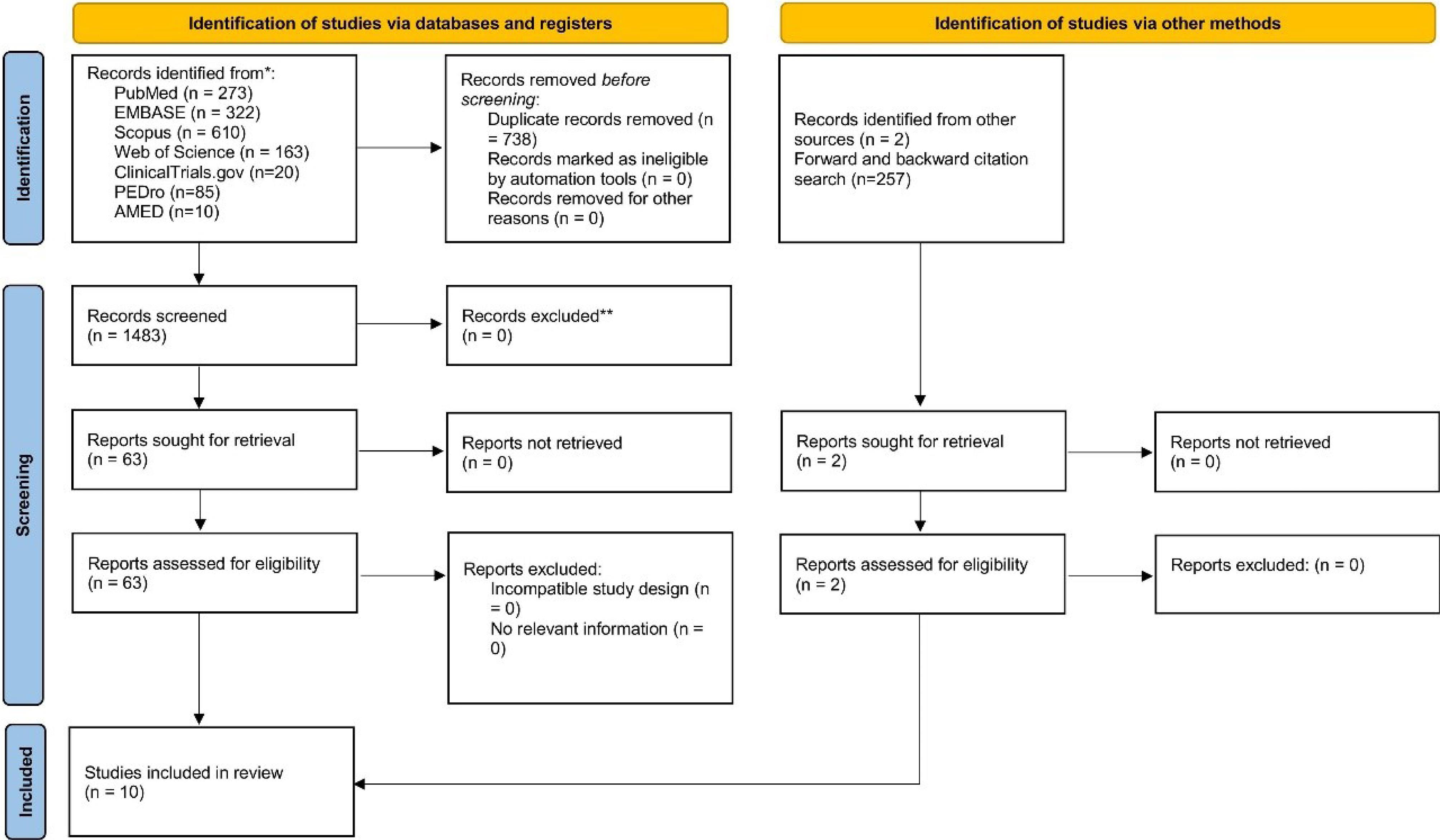
Figure 1.
Systematic Search of Reports
.
Systematic Search of Reports
Characteristics of Included Studies
The trials collectively involved 647 pregnant and postpartum women with back pain or pelvic girdle pain, conducted in various countries, including Egypt, Turkey, Iran, Thailand, India, and Poland. The mean age of participants ranged from 21.79 to 35.2 years. Gestational age varied across studies, with some interventions administered during the third trimester and others during the postpartum period. The duration of the interventions ranged from 1 day to 5 weeks. Nine studies, conducted across various countries and published between 2011 and 2023, were included in this meta-analysis. The studies included a mix of sample sizes and study designs, including randomized controlled trials (RCTs) and quasi-experimental studies. KT interventions were compared with various control conditions, including standard pregnancy care, placebo tape, pelvic exercises, exercise programs, and routine care.
Pain intensity and disability were commonly assessed using VAS, RMDQ, Oswestry Low Back Pain Disability Questionnaire, BPFS, and NPRS. The studies employed various outcome measures to evaluate the effectiveness of KT intervention in reducing pain intensity and disability levels in pregnant and postpartum women experiencing low back pain. The characteristics of the included studies are summarized in Table S2.
Effectiveness of Kinesio Tape Intervention
All included studies reported improvements in pain intensity and disability among participants receiving KT interventions compared to control groups. For example, Aalishahi et al18 in Iran observed reductions in pain intensity at multiple time points, though no significant change in disability was noted (P = 0.722). Sabbour and Omar20 in Egypt reported reductions in both pain intensity and disability, with a difference between the intervention and control groups (P< 0.01).
Kalinowski and Krawulska25 in Poland demonstrated reductions in pain intensity, particularly on days two and seven post-treatment, with P values less than 0.001 for these time points. Mohamed et al21 in Egypt similarly found that KT, combined with an exercise program, reduced pain intensity and disability compared to exercise alone (P= 0.001). Kaplan et al19 in Turkey reported superior outcomes for both pain and disability measures in the KT group (P < 0.001 for both), with greater improvements observed in the intervention group compared to the control.
Other studies, including those by Ordahan and Eriç Horasanlı22 in Turkey and Chamnankrom et al23 in Thailand, reported similar findings. Ordahan and Eriç Horasanlı22 found improvements in all outcome parameters in the KT group (P < 0.001), while Chamnankrom et al23 observed reductions in pain and disability, with P values ranging from 0.001 to 0.04 across measures.
Additionally, Rishi et al24 in India and Ahmed et al26 in Egypt demonstrated reductions in pain intensity and disability levels with KT compared to conventional physiotherapy or routine care (P values for both groups ≤ 0.001). Baraia et al27 in Egypt reported positive effects of KT in reducing postpartum back pain, fatigue, and disability (P ≤ 0.0001). Detailed outcome data, including P values for pain intensity and disability measures, can be found in Table S3.
Quality Assessment
The risk of bias assessment for the studies is summarized in Table S4. The majority of investigations showed some level of uncertainty concerning random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcomes assessments, incomplete outcome data, selective reporting, and other potential biases. Specifically, Aalishahi et al18 established high-risk blinding of participants and personnel, while Kalinowski et al,25 Kaplan et al,19 and Rishi et al24 exhibited high risks across multiple domains, including blinding of outcome assessment and incomplete outcome data. In contrast, Chamnankrom et al23 and Mohamed et al21 demonstrated relatively lower risks across all assessed areas. Ahmed et al26 and Baraia et al27 reported unknown risks across all domains due to insufficient information in their studies.
Meta-Analysis
Roland Morris Disability Questionnaire
Analysis of RMDQ scores across the included studies revealed a consistent trend favoring KT intervention. The pooled mean difference in RMDQ scores between the KT and control groups was statistically significant (MD = -4.47, 95% CI: -5.89 to -3.06). This indicates a substantial reduction in functional disability associated with low back pain in participants receiving KT therapy compared to those receiving usual care. However, considerable heterogeneity was observed across studies (χ2 = 155.36, df = 6, P < 0.00001, I2 = 96%), indicating variability in the effect sizes. Despite this heterogeneity, the overall effect of the interventions was statistically significant (Z = 6.21, P < 0.00001), supporting the efficacy of KT intervention in managing low back pain in postpartum women (See Figures 2A and 2B).
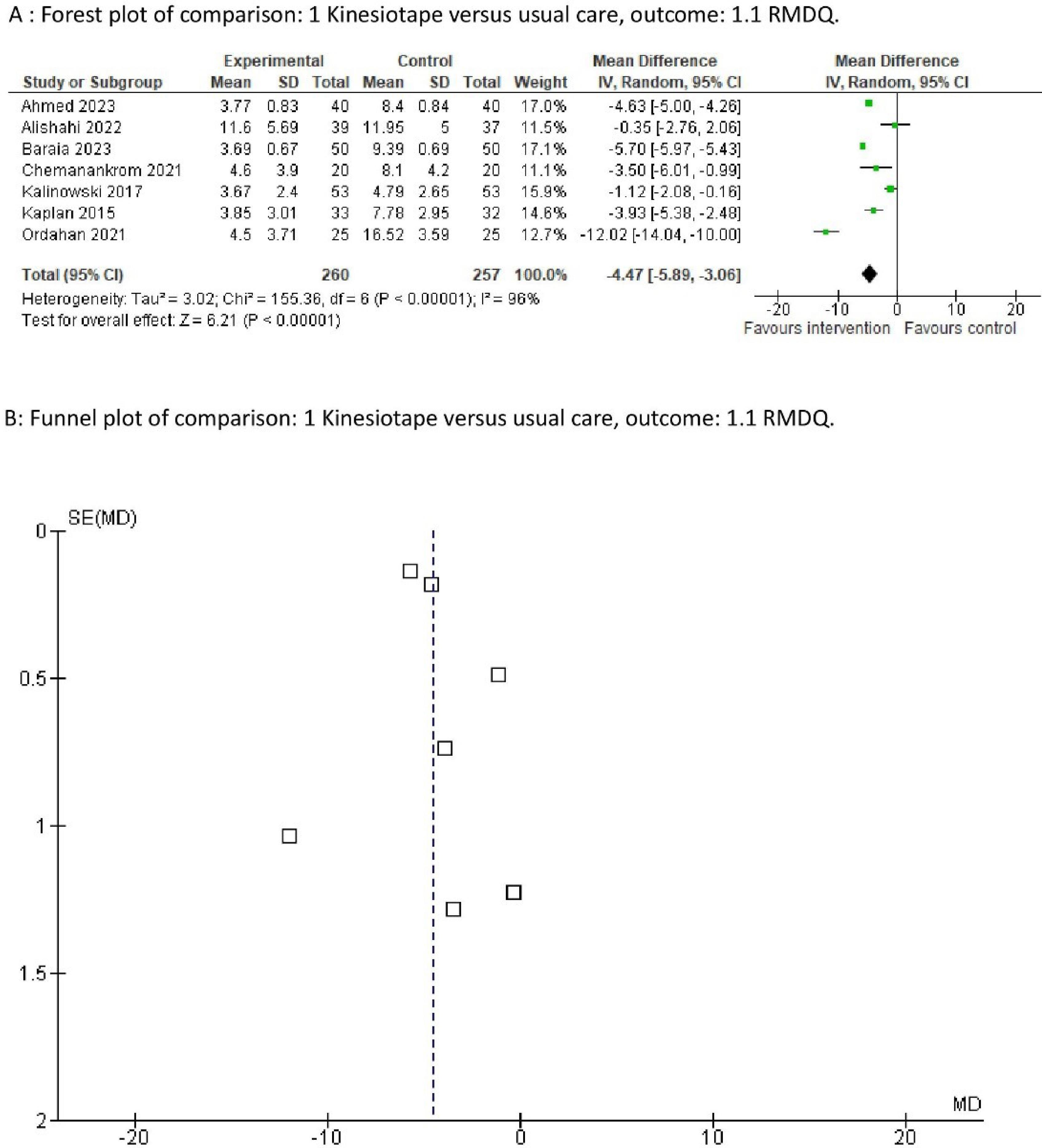
Figure 2.
Forest Plot and Funnel Plot of the Comparison of RMDQ Scores. Note. RMDQ: Roland Morris disability questionnaire
.
Forest Plot and Funnel Plot of the Comparison of RMDQ Scores. Note. RMDQ: Roland Morris disability questionnaire
Visual Analog Scales
Similarly, the analysis of VAS scores demonstrated a significant reduction in pain intensity following KT intervention. The pooled mean difference in VAS scores favored the KT group (MD = -4.47, 95% CI: -5.89 to -3.06), indicating a clinically significant decrease in pain levels among individuals treated with KT compared to those receiving standard care.
The findings of this meta-analysis suggest that KT therapy is an effective intervention for reducing both functional disability and pain intensity associated with low back pain. The consistent favorable outcomes across multiple studies provide robust evidence supporting the use of KT as an adjunctive treatment modality for low back pain management.
However, heterogeneity was observed across studies (χ2 = 153.31, df = 8, P < 0.00001, I2 = 95%), indicating variability in the effect sizes. Despite this, the overall effect of the intervention was statistically significant (Z = 24.33, P < 0.00001), further supporting the efficacy of KT intervention for low back pain management, including in postpartum women (See Figures 3A and 3B).
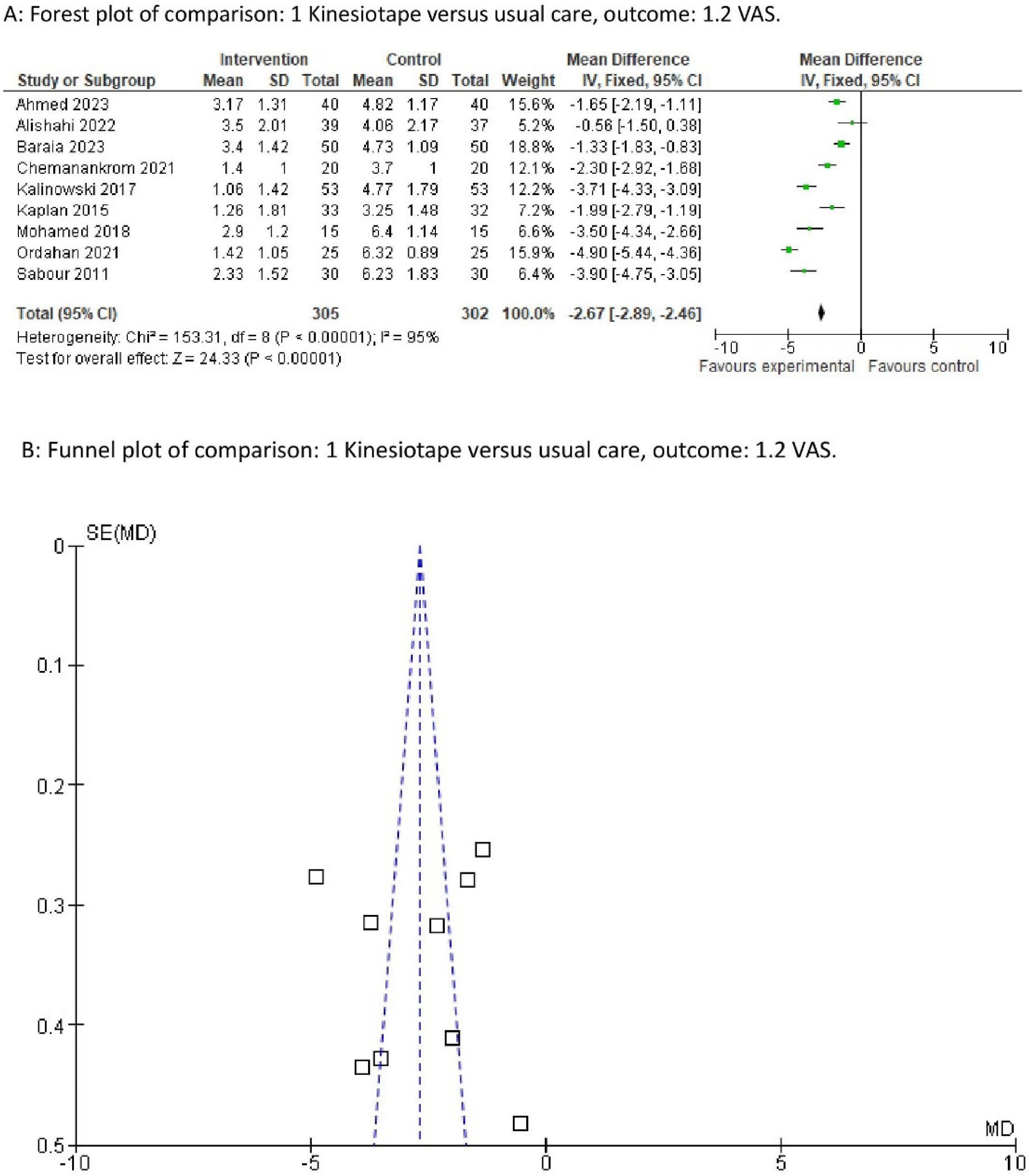
Figure 3.
Forest Plot and Funnel Plot of the Comparison of VAS Scores. Note. VAS: Visual analog scale
.
Forest Plot and Funnel Plot of the Comparison of VAS Scores. Note. VAS: Visual analog scale
The findings of this meta-analysis suggest that KT therapy is an effective intervention for reducing both functional disability and pain intensity associated with low back pain. While some studies included in the analysis were not exclusively focused on postpartum women, the consistent favorable outcomes across multiple populations provide robust evidence supporting the use of KT as an adjunctive treatment modality in the management of low back pain.
Discussion
A systematic review was conducted to assess the effectiveness of conservative management and KT methods on low back pain and pelvic girdle pain during and after pregnancy. The findings of this systematic review and meta-analysis indicate that KT intervention is effective in reducing both functional disability and pain intensity associated with low back pain among pregnant and postpartum women. The meta-analysis demonstrated a statistically significant reduction in RMDQ scores, indicating a substantial improvement in functional disability levels among participants receiving KT therapy compared to those receiving usual care. Similarly, a significant reduction was observed in pain intensity, as evidenced by the pooled mean difference in VAS scores, indicating a clinically relevant decrease in pain levels among individuals treated with KT compared to those receiving standard care. The consistent favorable outcomes across multiple studies provide evidence supporting the use of KT as an adjunctive treatment modality for managing low back pain during pregnancy and the postpartum period. These findings have significant implications for healthcare providers involved in antenatal and postpartum care, highlighting the potential benefits of incorporating KT therapy into routine management strategies for low back pain.
Our findings are in line with previous studies investigating the efficiency of KT in several patient populations with musculoskeletal conditions. Previous research has established the positive effects of KT in reducing pain and improving functional outcomes in situations such as chronic back pain. For example, Xue et al28 conducted a systematic review and meta-analysis to evaluate the efficacy and safety of KT in the treating of low back pain during pregnancy. They identified seven randomized clinical trials with 444 patients, and the results indicated that KT intervention significantly improved low back pain and dysfunction compared to the control group, as evidenced by decreases in both VAS and RMDQ scores.
Additionally, KT intervention was found to be effective in improving low back pain during the second and third trimesters of pregnancy. The study concluded that KT has a positive effect on improving lower back pain during pregnancy and suggested that future research should focus on prevention and treatment strategies to enhance women’s health. Chen et al29 conducted a meta-analysis to compare the efficacy and safety of conservative care strategies for pregnancy-related low back pain. Their study included a comprehensive search of multiple databases up to November 2019, identifying 23 studies for qualitative synthesis and 18 RCTs for network meta-analysis. They found that both progressive muscle relaxation therapy and KT were associated with reduced pain intensity compared to placebo, with moderate-quality evidence supporting progressive muscle relaxation therapy and low-quality evidence supporting KT. The study concluded that both progressive muscle relaxation therapy and KT could help decrease pain, while transcutaneous electrical nerve stimulation may improve physical function in patients with low back pain during pregnancy.29
In contrast to the findings of Xue et al28 and Chen et al,29 which offered valuable insights into the efficacy of KT for low back pain during pregnancy, our systematic review and meta-analysis extend this knowledge by incorporating more recent studies and providing a comprehensive analysis of the effectiveness of KT intervention across diverse populations and settings. Additionally, our study contributes new insights into the role of KT in reducing both pain intensity and disability levels among pregnant and postpartum women, further supporting its role as an adjunctive treatment modality for managing low back pain.
In contrast, Koukoulithras et al7 conducted a systematic review and meta-analysis to evaluate the effectiveness of non-pharmaceutical interventions in reducing pregnancy-related low back pain. They identified 13 RCTs meeting their inclusion criteria. Various interventions such as exercise, manipulation, ear acupuncture, KT, transcutaneous electrical nerve stimulation, and neuroemotional techniques, were analyzed. However, KT did not significantly reduce pregnancy-related low back pain compared to typical care or sham treatment.7 The differences in results between our study and that of Koukoulithras et al7 can be attributed to several factors. Our review specifically focused on KT interventions for back pain and pelvic girdle pain in pregnant and postpartum women, including 10 studies (7 RCTs and 3 quasi-experimental). In contrast, Koukoulithras et al7 analyzed 13 RCTs with a broader range of non-pharmaceutical interventions, including exercise, manipulation, and KT. This broader focus might dilute the specific effects of KT when compared to standard care or sham treatments. Furthermore, differences in the methodological approaches used such as criteria for assessing study quality, data extraction, and statistical analysis may have contributed to the varying results. Our review employed detailed quality assessments and accounted for variability, which might differ from the approach taken by Koukoulithras et al.7 Additionally, publication bias and random variability may further explain the differences in findings.
The present study extends the existing evidence to pregnant and postpartum women experiencing low back pain, providing further support for the use of KT in this population. Low back pain is a common condition among pregnant women, arising from changes in skeletal, muscular, and nervous systems, as well as alterations in body conditions, which affects their quality of life and increases disability.1,2 Factors such as young maternal age, advanced maternal age, and prolonged periods of standing and sitting throughout the day are key contributors to the prevalence of pregnancy-related low back pain.30 Younger women may experience back pain due to physical immaturity or muscle weakness, while older women may be more susceptible due to age-related changes in the spine and muscles.3 Additionally, a significant portion of the treatment-related leave expenses during pregnancy is attributed to low back pain.31 The high recurrence rate in subsequent pregnancies emphasizes the need for developing effective treatment programs for this condition. Despite these figures, it is estimated that over 50% of pregnant women receive minimal intervention from healthcare providers.32
Based on the findings of this systematic review and meta-analysis, healthcare workers should consider incorporating KT therapy as part of a multimodal approach to managing low back pain during pregnancy and the postpartum period. Future studies should focus on determining the optimal application techniques, dosages, and duration of KT therapy to maximize its therapeutic benefits for this population. Furthermore, well-designed RCTs with larger sample sizes and longer follow-up periods are necessary to further investigate the efficacy and long-term effects of KT intervention in pregnant and postpartum women with low back pain.
Limitations
Despite the strengths of this review, several limitations should be acknowledged. First, the heterogeneity observed across studies may limit the generalizability of our findings. Variability in participant characteristics, intervention protocols, and outcome measures may have contributed to the observed heterogeneity. Second, the risk of bias in the included studies, particularly regarding the blinding of participants and personnel and the blinding of outcome assessments, may affect the validity of the results. A significant number of the included studies (7 out of 10) were assessed as having an unknown or high risk of bias. We acknowledge that the inclusion of these studies may have impacted the overall findings, potentially overstating the effectiveness of KT interventions for back pain and pelvic girdle pain. However, we included these studies to provide a comprehensive analysis of the available evidence and avoid selection bias by excluding potentially relevant data. Excluding these studies could have limited the scope of our findings and might not have fully represented the real-world clinical context, where study quality often varies.
We believe that while they contribute valuable data, the direction of their potential bias-likely overestimating treatment effects due to issues like lack of blinding-suggests that the treatment effect of KT may be more moderate than our pooled estimates indicate. This highlights the need for a cautious interpretation of the findings and calls for further high-quality, blinded trials to confirm the efficacy of KT in this population.
Lastly, the inclusion of only published studies may introduce publication bias, potentially leading to an overestimation of the treatment effects.
Conclusion
In conclusion, our study underscores the effectiveness of KT interventions in reducing pain intensity and disability levels among pregnant and postpartum women experiencing low back pain. These findings align with previous research demonstrating the potential benefits of KT across various clinical conditions. However, our study also highlights the need for further investigation to clarify the optimal use of KT, particularly in comparison to sham or usual care interventions. While our findings contribute to the growing body of evidence supporting the efficacy of KT, additional high-quality RCTs are needed to provide more definitive conclusions regarding its clinical utility. Nonetheless, KT represents a promising adjunctive treatment modality for managing low back pain in pregnant and postpartum populations, offering potential benefits for improving maternal well-being and quality of life.
Authors’ Contribution
Conceptualization: Vahideh Toopchizadeh.
Data curation: Kimia Motlagh.
Formal analysis: Vahideh Toopchizadeh.
Funding acquisition: Fereshteh Jamali.
Investigation: Vahideh Toopchizadeh.
Methodology: Yasaman Mirzazadeh.
Project administration: Yasaman Mirzazadeh.
Resources: Vahideh Toopchizadeh.
Software: Yasaman Mirzazadeh.
Supervision: Neda Dolatkhah.
Validation: Kimia Motlagh.
Visualization: Kimia Motlagh.
Writing-original draft: Kimia Motlagh.
Writing-review & editing: Fereshteh Jamali.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
This study was approved by the ethical committee of Tabriz University of medical seciences (Ethics No. IR.TBZMED.REC.1403.335).
Supplementary Files
Supplementary file 1 contains Tables S1-S4.
(pdf)
References
- Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J 2010; 19(12):2075-94. doi: 10.1007/s00586-010-1502-y [Crossref] [ Google Scholar]
- Vermani E, Mittal R, Weeks A. Pelvic girdle pain and low back pain in pregnancy: a review. Pain Pract 2010; 10(1):60-71. doi: 10.1111/j.1533-2500.2009.00327.x [Crossref] [ Google Scholar]
- Bryndal A, Glowinski S, Majchrzycki M. Influence of pregnancy on the occurrence of lumbar spine pain in polish women: a retrospective study. J Pers Med 2022; 12(3):357. doi: 10.3390/jpm12030357 [Crossref] [ Google Scholar]
- Katonis P, Kampouroglou A, Aggelopoulos A, Kakavelakis K, Lykoudis S, Makrigiannakis A. Pregnancy-related low back pain. Hippokratia 2011; 15(3):205-10. [ Google Scholar]
- Steiger F, Wirth B, de Bruin ED, Mannion AF. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur Spine J 2012; 21(4):575-98. doi: 10.1007/s00586-011-2045-6 [Crossref] [ Google Scholar]
- Sahebozamani M, Siamaki Gharieh Safa R, Ahrari MN. Abdominal muscles activity in health and hyperlordose groups during prone bridging stabilization exercise. Olympic 2011; 18(4):99-110. [ Google Scholar]
- Koukoulithras I Sr, Stamouli A, Kolokotsios S, Plexousakis M Sr, Mavrogiannopoulou C. The effectiveness of non-pharmaceutical interventions upon pregnancy-related low back pain: a systematic review and meta-analysis. Cureus 2021; 13(1):e13011. doi: 10.7759/cureus.13011 [Crossref] [ Google Scholar]
- Maia LB, Amarante LG, Vitorino DF, Mascarenhas RO, Lacerda ACR, Lourenço BM. Effectiveness of conservative therapy on pain, disability and quality of life for low back pain in pregnancy: a systematic review of randomized controlled trials. Braz J Phys Ther 2021; 25(6):676-87. doi: 10.1016/j.bjpt.2021.06.007 [Crossref] [ Google Scholar]
- Adibi P, Kalani N, Razavi BM, Mehrpour S, Zarei T, Malekshoar M. Pharmacological and non-pharmacological methods of pain control in women undergoing caesarean section: a narrative review. Iran J Obstet Gynecol Infertil 2022; 25(7):91-112. doi: 10.22038/ijogi.2022.21138 [Crossref] [ Google Scholar]
- Bastiaenen CH, de Bie RA, Wolters PM, Vlaeyen JW, Leffers P, Stelma F. Effectiveness of a tailor-made intervention for pregnancy-related pelvic girdle and/or low back pain after delivery: short-term results of a randomized clinical trial [ISRCTN08477490]. BMC Musculoskelet Disord 2006; 7:19. doi: 10.1186/1471-2474-7-19 [Crossref] [ Google Scholar]
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 2009; 151(4):W65-94. doi: 10.7326/0003-4819-151-4-200908180-00136 [Crossref] [ Google Scholar]
- Chiarotto A, Maxwell LJ, Ostelo RW, Boers M, Tugwell P, Terwee CB. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain 2019; 20(3):245-63. doi: 10.1016/j.jpain.2018.07.009 [Crossref] [ Google Scholar]
- Katz J, Melzack R. McGill pain questionnaire. In: Maggino F, ed. Encyclopedia of Quality of Life and Well-Being Research. Cham: Springer; 2020. p. 1-4. 10.1007/978-3-319-69909-7_1748-3.
- Morris D, Jones D, Ryan H, Ryan CG. The clinical effects of Kinesio® Tex taping: a systematic review. Physiother Theory Pract 2013; 29(4):259-70. doi: 10.3109/09593985.2012.731675 [Crossref] [ Google Scholar]
- Lim EC, Tay MG. Kinesio taping in musculoskeletal pain and disability that lasts for more than 4 weeks: is it time to peel off the tape and throw it out with the sweat? A systematic review with meta-analysis focused on pain and also methods of tape application. Br J Sports Med 2015; 49(24):1558-66. doi: 10.1136/bjsports-2014-094151 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71 [Crossref] [ Google Scholar]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366:l4898. doi: 10.1136/bmj.l4898 [Crossref] [ Google Scholar]
- Aalishahi T, Maryam-Lotfipur-Rafsanjani S, Ghorashi Z, Sayadi AR. The effects of Kinesio tape on low back pain and disability in pregnant women. Iran J Nurs Midwifery Res 2022; 27(1):41-6. doi: 10.4103/ijnmr.IJNMR_291_20 [Crossref] [ Google Scholar]
- Kaplan Ş, Alpayci M, Karaman E, Çetin O, Özkan Y, İlter S. Short-term effects of Kinesio taping in women with pregnancy-related low back pain: a randomized controlled clinical trial. Med Sci Monit 2016; 22:1297-301. doi: 10.12659/msm.898353 [Crossref] [ Google Scholar]
- Sabbour A, Omar H. The effect of Kinesio taping therapy augmented with pelvic tilting exercises on low back pain in primigravidas during the third trimester. Bull Fac Phys Ther Cairo Univ 2011; 16(1):53-61. [ Google Scholar]
- Mohamed EA, El-Shamy FF, Hamed H. Efficacy of Kinesio tape on functional disability of women with postnatal back pain: a randomized controlled trial. J Back Musculoskelet Rehabil 2018; 31(1):205-10. doi: 10.3233/bmr-170827 [Crossref] [ Google Scholar]
- Ordahan B, Eriç Horasanlı J. Effectiveness of Kinesio taping in pregnant women with sacroiliac joint pain: a randomised controlled study. Int J Clin Pract 2021; 75(9):e14432. doi: 10.1111/ijcp.14432 [Crossref] [ Google Scholar]
- Chamnankrom M, Manimmanakorn N, Manimmanakorn A, Kongwattanakul K, Hamlin MJ. Effects of elastic tape in pregnant women with low back pain: a randomized controlled trial. J Back Musculoskelet Rehabil 2021; 34(1):111-9. doi: 10.3233/bmr-200094 [Crossref] [ Google Scholar]
- Rishi P, Yadav J, Anand P, Yadav B. Efficacy of Kinesio taping among females with postpartum low back pain - a quasi-experimental study. J Clin Diagn Res 2022; 16(2):YC01-4. doi: 10.7860/jcdr/2022/51643.15975 [Crossref] [ Google Scholar]
- Kalinowski P, Krawulska A. Kinesio taping vs placebo in reducing pregnancy-related low back pain: a cross-over study. Med Sci Monit 2017; 23:6114-20. doi: 10.12659/msm.904766 [Crossref] [ Google Scholar]
- Ahmed AH, Hassan SI, Shamekh Taman AH. Effect of Kinesio tape on postpartum low back pain and functional disability in women after cesarean section. Assiut Sci Nurs J 2023; 11(37):141-52. doi: 10.21608/asnj.2023.207977.1579 [Crossref] [ Google Scholar]
- Baraia ZA, Thabet HA, Abu Almakarem AS, El-Sayed Atwa AM. Impact of instructional guidelines regarding Kinesio tape on postpartum back pain, fatigue, and disability in women with cesarean section. Egypt J Health Care 2023; 14(4):479-94. doi: 10.21608/ejhc.2023.327342 [Crossref] [ Google Scholar]
- Xue X, Chen Y, Mao X, Tu H, Yang X, Deng Z. Effect of Kinesio taping on low back pain during pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth 2021; 21(1):712. doi: 10.1186/s12884-021-04197-3 [Crossref] [ Google Scholar]
- Chen L, Ferreira ML, Beckenkamp PR, Caputo EL, Feng S, Ferreira PH. Comparative efficacy and safety of conservative care for pregnancy-related low back pain: a systematic review and network meta-analysis. Phys Ther 2021; 101(2):pzaa200. doi: 10.1093/ptj/pzaa200 [Crossref] [ Google Scholar]
- Rabiee M, Sarchamiee N. Frequency of low back pain in each pregnancy trimester and its related factors in pregnant women visiting Shaheed Mostafa Khomeini hospital in 2015. Iran J Obstet Gynecol Infertil 2018; 20(12):32-9. doi: 10.22038/ijogi.2017.10427 [Crossref] [ Google Scholar]
- Sydsjö A, Sydsjö G, Kjessler B. Sick leave and social benefits during pregnancy--a Swedish-Norwegian comparison. Acta Obstet Gynecol Scand 1997; 76(8):748-54. doi: 10.3109/00016349709024341 [Crossref] [ Google Scholar]
- Liddle SD, Pennick V. Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database Syst Rev 2015; 2015(9):CD001139. doi: 10.1002/14651858.CD001139.pub4 [Crossref] [ Google Scholar]