Biomed Res Bull. 1(1):38-41.
doi: 10.34172/biomedrb.2023.08
Case Report
Eosinophilic Annular Erythema as a Subset of Wells Syndrome or a Distinct Entity: Report of Two Cases
Hediyeh Ehteshami 1, Ilgar Amjadi 1, Leila-Sadat Hatamnezhad 1, 2, * 
Author information:
1Department of Dermatology, Sina Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
2Department of Dermatology, Kuhkamari Hospital, Marand-Iran
Abstract
Eosinophilic annular erythema (EAE) is an uncommon acute eosinophilic dermatosis of unknown etiology. Urticarial papules and plaques as pruritic lesions appear in annular and arcuate forms on the trunk and proximal limbs and rarely affect the face. In histopathological diagnosis, EAE has typical features, including acute dermal inflammatory infiltrate with abundant eosinophils and lymphocytes around arteries. In spite of no clear treatment, the findings indicated the positive effects of systemic corticosteroid, hydroxychloroquine, and Ultraviolet B therapy along with recurrences. Two patients have been elected in the present study. The first patient was a middle-aged diabetic female with urticarial papules and plaques around the pelvis and proximal thighs that had active borders with improved centers. We started with 400 mg of hydroxychloroquine and 25 mg of prednisone for the patient whose lesions were subsided during the first week. The second consulted patient was a 41-year-old female without a history of previous illness with four months of painful, pruritic, and violaceous plaques on the back of the trunk. In histopathology, dermal inflammatory infiltrate with abundant eosinophils was observed in the dermis. Corticosteroids and hydroxychloroquine were prescribed with the diagnosis of EAE for this patient as well.
Keywords: Wells syndrome, Eosinophilic annular erythema, Case report
Copyright and License Information
© 2023 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Eosinophilicannular erythema (EAE) is an uncommon disease, which previously was cured as a subset of Wells syndrome and was mostly reported in children but rarely in adults. However, EAE is characterized by recurrent urticarial painful and pruritic plaques which are starting to improve from the center, making figurate shapes, and disappearing without leaving the scar and residual dyspigmentation.
Case Presentation
Case I
The first patient was a 51-year-old diabetic woman with a history of asthma and breath shortness who was referred because of painful violaceous urticarial plaques on the flanks, pelvis, and proximal thighs. Some plaques were in annular form, improving from the center with a bruise similar to an appearance, and there was a subtle annular scale on some lesions. Plaques have been stable since the time of occurrence and have not responded to the full-dose oral antihistamine. The patient has had anemia resistant to treatment with hemoglobin of around 10 g/dL. Mild leukocytosis with eosinophilia (the range between 1500-3000) was detected during the sixth follow-up periods. The mild resistant anemia with hemoglobin of about 10 g/dL was always noticed, and the stool exam was negative for parasite assay in three quarters.
The test results were negative for central nervous system problems and neuropathy, and there was no history of arterial and venous thrombosis. Her chest X-ray, abdomen and pelvis computerized tomography scan, and spirometry were all normal, and there was no evidence of connective tissue diseases. Bone marrow biopsy showed cellular marrow with an increased number of megakaryocytes and a significant increase in the number of eosinophils. Furthermore, her liver and spleen sonography was normal, no organomegaly and abdominal free liquid were found, and her kidneys had normal size without any stone and hydronephrosis. In echocardiography, the parameters such as heart size, valves, atria, and ventricles volume were normal, ejection fraction was 60%, and there was no evidence of cardiomyopathy and hypertrophy. Due to chronic and persistent eosinophilia, the platelet-derived growth factor receptor-alpha (FIP1L1-PDGFRA) fusion gene was not identified via polymerase chain reaction of peripheral blood. Moreover, due to the clinical and laboratory panel for this patient, several differential diagnoses were suggested, including EAE, Wells syndrome, lupus tumidus, urticarial vasculitis, Jessner’s lymphocytic infiltrate, and pre-bullous pemphigoid
The observed syndromes in histopathology included epidermal acanthosis, parakeratosis, pustulation containing eosinophils, dermal edema, perivascular and interstitial eosinophilic rich infiltration, and collection of abundant eosinophilic granules with the extension to subcutis.
We did not find any reactive causes such as hypersensitivity diseases, infections, malignancies, or the like. Further, there was not any end organ damage in the one-year follow-up period. Figure 1 presents all of the above possible diagnoses of EAE.
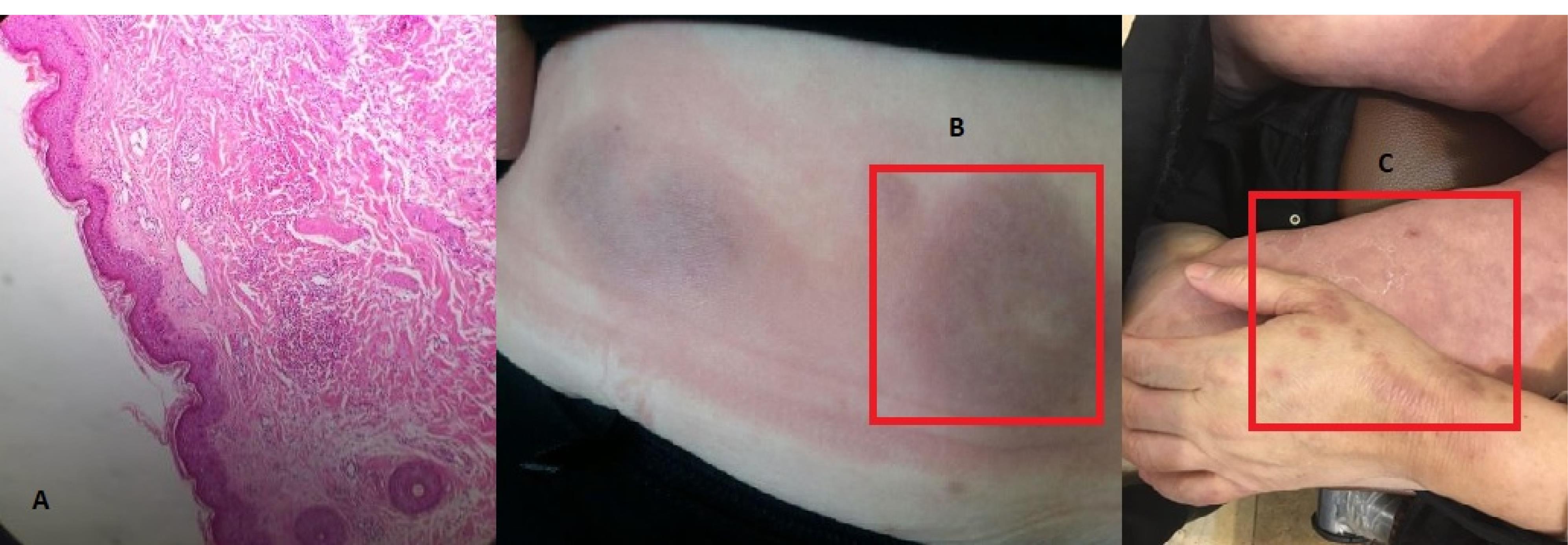
Figure 1.
(a) Dermal edema with perivascular and interstitial eosinophilic infiltrate; (b) and (c) Infiltrative plaques with bruise like appearance over the flanks and thighs.
.
(a) Dermal edema with perivascular and interstitial eosinophilic infiltrate; (b) and (c) Infiltrative plaques with bruise like appearance over the flanks and thighs.
Hydroxychloroquine 400 (mg/d) and prednisolone 25 (mg/d) were initially started. The lesions had begun to improve within one week, and gradually we tapered the dose of prednisolone. Occasional recurrences were seen at doses close to 7.5 (mg/d), and despite the addition of colchicine, no change was made in response, and it seemed that the plaques are flowed down only by adding the dose of prednisolone (Table 1).
Table 1.
Blood Information of Case I and Case II
|
Lab Test
|
Case I
|
Case II
|
Normal
|
| WBC |
10-16 *1000 |
8-10 *1000 |
4-10 *1000 |
| Hb |
11 |
14 |
12-17 |
| MCV |
78 |
96 |
80-100 |
| MCH |
24-60 |
29 |
27-32 |
| PLT |
552 *1000 |
231 *1000 |
150-500 *1000 |
| Eosinophil |
27% = 3 |
1/9 |
0.5-0.9 |
| ESR |
71 |
25 |
Lower 15 |
| CRP |
Negative |
Negative |
Lower 6 |
| IGE |
375 |
- |
2-100 |
| FBS |
- |
78 |
70-116 |
| TSH |
- |
1.1 |
0.2- 4.2 |
| T4 |
- |
15.3 |
4-12.3 |
| LDH |
260 |
316 |
Lower 480 |
| S/E |
Negative |
Negative |
|
| ANA |
Negative |
Negative |
|
| P-ANCA |
Negative |
Negative |
|
| C-ANCA |
Negative |
Negative |
|
| RF |
Negative |
Negative |
|
| U/A |
Normal |
Normal |
|
Note. WBC, white blood cell; Hb, hemoglobin; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; PLT, platelet count; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; IGE, immunoglobulin E; FBS, fasting blood sugar; TSH; thyroid stimulating hormone; T4, thyroxine; HDL, high-density lipoprotein; SE, stool exam; ANA, antinuclear antibody; P-ANCA, perinuclear antineutrophil cytoplasmic antibodies; C-ANCA, cytoplasmic antineutrophil cytoplasmic antibodies; RF, rheumatoid factor; U/A, urinalysis.
Case II
The second patient who was referred because of Wells syndrome was a 41-year-old white woman without any disease history but a 4-month history of painful and itchy erythematous and violaceous plaques at the back of the trunk. The patient’s lesions were polycyclic, arcuate, and somehow petaloid with a scalloped border which were improved centrally by leaving hyperpigmentation. There were also small papules and plaques in the proximal upper and lower limbs, but there was no facial involvement anymore. Furthermore, electrolytes, complements, hepatitis serology, and stool tests all were normal or negative (Figure 2).

Figure 2.
(a) Dense infiltration of lymphocytes and eosinophils with collections eosinophilic granules; (b) Petaloid and figurate plaques with central healing.
.
(a) Dense infiltration of lymphocytes and eosinophils with collections eosinophilic granules; (b) Petaloid and figurate plaques with central healing.
The chest and abdominal computerized tomography scan were done, and there was not any underlying disorder. In the biopsy of the trunk lesions, the epidermis was unremarkable, and eosinophilic infiltrate was evident in the upper and deep dermis and also around the vessels. The patient was treated with prednisolone 15 mg/d, hydroxychloroquine 400 mg/d, indomethacin 25 mg/d, and loratadine 10 mg/d, which exhibited a slight improvement in the lesions (Table 1).
Discussion
EAE, previously defined as a subset of Wells syndrome, is a rare and newly diagnosed disease that was first described in 2000.1-5 Most of the reported patients are children, and it rarely occurs in adults. Wells syndrome, also known as eosinophilic cellulitis, with inflammatory dermatitis and acute erythematous plaques is composed of collagen-coated eosinophilic granules, so-called flame figures.6,7 In contrast, EAE is characterized by eosinophilic infiltration and lymphocytes around vessels and throughout the dermis.4 The characteristic manifestation of EAE is recurrent erythematous to violaceous papules and plaques which are pruritic or painful and are mainly seen on the trunk, proximal limbs, and face.2 The plaques are generally figurate with active margins, gradually clear from the center, and disappear in the form of hyperpigmentation or burgundy color without atrophy or scar.6 Although EAE is considered a self-limiting condition, it is resistant to therapy and recurs episodically. Despite the uncertain etiology, it may be a reaction to an increased hypersensitivity to an unknown antigen.2 EAE may be associated with chronic conditions such as autoimmune thyroid disorders (hyperthyroidism and hypothyroidism), chronic borreliosis, chronic Helicobacter pylori gastritis, chronic liver diseases, diabetes mellitus, and hepatitis C.7 Increasing the eosinophil level of serum can be divided into the primary hypersensitivity due to immune system disorders and secondary hyper-eosinophilia that can be idiopathic or caused by infection, allergy, vasculitis, drugs, and lymphoma.8,9 Hypereosinophilic syndrome, which is an idiopathic eosinophilia subtype, includes persistent eosinophilia of peripheral blood over 1500/mm3 for longer than 6 months with symptoms of organ involvement.8
The most important causes of eosinophilia are allergies, vasculitis, malignancies, and some parasitic, bacterial, and fungal infections. Some medications associated with eosinophilia include allopurinol, carbamazepine, and some antibiotics.8 Among allergies and vasculitis, eosinophilic lung diseases are more prominent which include chronic and acute pneumonia, bronchopulmonary aspergillosis, and the Churg–Strauss syndrome.8 Generally, the diagnosis of eosinophilia requires complete patient history, clinical examinations, history of previous illnesses, list of medications, and laboratory tests such as multiple stool exams to detect infectious parasitic, chest X-ray, and serological tests for infectious pathogens.
So far, several test treatments for these patients have been prednisolone, hydroxychloroquine, loratadine, acitretin, ivermectin, anastrozole, indomethacin, sulfasalazine, methotrexate, cyclosporine, leflunomide, and lumiracoxib.1,6,7 Most of these treatments have been associated with recurrence after treatment discontinuation.2,6 Currently, the first line of treatment is prednisolone and hydroxychloroquine.
Conclusion
EAE is a disease with unknown etiology, and it is not clear yet whether this disease is a subset of Wells disease or not. By putting signs together along with clinical and histopathology features, it seems that EAE is a distinct and different disease that is related to the dense eosinophilic infiltrate of the skin with or without eosinophilia of peripheral blood.
Authors’ Contribution
Conceptualization: Hadiyeh Ehteshami.
Formal Analysis: Hediyeh Ehteshami, Ilgar Amjadi.
Funding Acquisition: Self Fund.
Methodology: Hediyeh Ehteshami, Ilgar Amjadi, Leila-Sadat Hatamnezhad.
Supervision: Leila-Sadat Hatamnezhad.
Writing — Original Draft: Hediyeh Ehteshami, Ilgar Amjadi.
Writing — Review & Editing: Leila-Sadat Hatamnezhad.
Competing Interests
None to be declared.
Ethical Approval
Informed consent was obtained from both patients for publication of this report.
References
- Awosika O, Totoraitis K, Eleryan M, Rengifo-Pardo M, Ehrlich A. A case of eosinophilic annular erythema as a presenting sign for autoimmune hepatitis. JAAD Case Rep 2018; 4(1):84-6. doi: 10.1016/j.jdcr.2017.01.007 [Crossref] [ Google Scholar]
- Boyer DF. Blood and bone marrow evaluation for eosinophilia. Arch Pathol Lab Med 2016; 140(10):1060-7. doi: 10.5858/arpa.2016-0223-RA [Crossref] [ Google Scholar]
- Heras MO, Muñoz NP, Sancho MI, Millet PU. Eosinophilic annular erythema in adults: report of two cases and review of the literature. An Bras Dermatol 2017; 92(5 Suppl 1):65-8. doi: 10.1590/abd1806-4841.20176373 [Crossref] [ Google Scholar]
- Howes R, Girgis L, Kossard S. Eosinophilic annular erythema: a subset of Wells’ syndrome or a distinct entity?. Australas J Dermatol 2008; 49(3):159-63. doi: 10.1111/j.1440-0960.2008.00456.x [Crossref] [ Google Scholar]
- Nakazato S, Fujita Y, Shinkuma S, Nomura T, Shimizu H. Eosinophilic annular erythema is clinically characterized by central pigmentation reflecting basal melanosis: a clinicopathological study of 10 cases. J Eur Acad Dermatol Venereol 2017; 31(11):1916-23. doi: 10.1111/jdv.14350 [Crossref] [ Google Scholar]
- Tefferi A, Gotlib J, Pardanani A. Hypereosinophilic syndrome and clonal eosinophilia: point-of-care diagnostic algorithm and treatment update. Mayo Clin Proc 2010; 85(2):158-64. doi: 10.4065/mcp.2009.0503 [Crossref] [ Google Scholar]
- Thomas L, Fatah S, Nagarajan S, Natarajan S. Eosinophilic annular erythema: successful response to ultraviolet B therapy. Clin Exp Dermatol 2015; 40(8):883-6. doi: 10.1111/ced.12668 [Crossref] [ Google Scholar]
- Wallis L, Gilson RC, Gilson RT. Dapsone for recalcitrant eosinophilic annular erythema: a case report and literature review. Dermatol Ther (Heidelb) 2018; 8(1):157-63. doi: 10.1007/s13555-017-0214-1 [Crossref] [ Google Scholar]
- Williams KW, Milner JD, Freeman AF. Eosinophilia associated with disorders of immune deficiency or immune dysregulation. Immunol Allergy Clin North Am 2015; 35(3):523-44. doi: 10.1016/j.iac.2015.05.004 [Crossref] [ Google Scholar]