Biomed Res Bull. 1(4):122-129.
doi: 10.34172/biomedrb.2023.24
Original Article
Obsessive-Compulsive Disorder: Temperament and Character Subscales and Personality Development
Alireza Farnam 1, #  , Afra Pirahmadi 1, #, Amirreza Azarmnia 1, * , Masumeh Zamanlu 2, *
, Afra Pirahmadi 1, #, Amirreza Azarmnia 1, * , Masumeh Zamanlu 2, *
Author information:
1Self-awareness Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
2Neuroscience Research Center, Qom University of Medical Sciences, Qom,Iran
#These authors are contributed equally to this work.
Abstract
Background:
Personality backgrounds related to obsessive-compulsive disorder (OCD) have been investigated for several decades. However, the subscales (lower-order traits or component facets) of temperament and character have rarely been mentioned, which are the aims of evaluation in the current cross-sectional study.
Methods:
Fifty-one OCD patients (aged 30.59±9.49 years old) diagnosed based upon Diagnostic and Statistical Manual of Mental Disorder-IV criteria and 53 age- and gender-matched control subjects free of psychiatric diseases (aged 30.23±9.41 years old) were incorporated. Patients and controls completed the Temperament and Character Inventory (TCI-125). OCD patients completed the inventory for the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) as well.
Results:
The scores of the TCI seven factors and subscales were compared in OCD patients and control subjects. OCD patients showed a highly significant increase in harm avoidance, anticipatory worry, fear of uncertainty, shyness, fatigability, and persistence. On the other hand, a highly significant decrease was observed in attachment self-directedness, responsibility, purposefulness, resourcefulness, spontaneity, cooperativeness, tolerance, compassion, principledness, transpersonal identification, and personality development.
Conclusion:
It is concluded that significant temperament and character differences in OCD patients existed, which could be incorporated for further comprehension of OCD and more specific pharmacotherapies and psychotherapies, especially psychotherapies focusing on personality development.
Keywords: Personality dimensions, Cloninger’s theory, Anxiety disorders, Behavior mechanisms
Copyright and License Information
© 2024 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Obsessive-compulsive disorder (OCD) is a common mental disorder that substantially disables the afflicted individuals in family, occupational, and social functions. The disorder is characterized by intrusive thoughts and repetitive and ritual behaviors; however, the diagnosis implies considerable heterogeneity, and models have been introduced for the dimensional description of OCD.1-5 Moreover, it has been shown that intrusive thoughts (obsessions) and even compulsions are not uncommon in the normal population, and therefore the disorder occurs when obsessions and compulsions impose suffering and dysfunction6-8; thus, it is suggested that “an obsessive–compulsive spectrum grouping of disorders be included in the Diagnostic and Statistical Manual of Mental Disorders (DSM‐V)”.9
Similarly, individual differences based on personality models in OCD have been evaluated in previous research, including dimensional personality models. The previously studied personality models include categorically defined personality disorders,10-13 normal personality models, including psychoticism, extraversion, and neuroticism) model of personality,14 the Big Five personality traits (by the Neo Five-Factor Inventory),15,16 and Gray’s theory of personality.17,18 Cloninger’s psychobiological model of personality has been assessed in OCD patients in several studies, mainly insisting on higher scores of harm avoidance and lower scores of self-directedness and cooperativeness.19-29 Only one classic study utilizing the Tridimensional Personality Model of Cloninger has reported the subscales of temperament, concluding that fear of uncertainty (the second subscale of harm avoidance) showed the highest difference among other subscales.30
The psychiatry textbook claims that “until recently, access to the inner mechanisms of human mental functions was severely limited. Psychiatrists often skipped efforts to describe and understand healthy mental functioning and focused on mental disorders”.31,32 The personality model proposed by Cloninger, the temperament and character model of personality, has been demonstrated to be beneficial and reliable in descriptions and predictions of thoughts, emotions, behaviors, and the clinical course of psychiatric disorders. This model was introduced based on extensive evidence, including person-centered analyses of general populations from various cultures. These studies illustrate the strengths and vulnerabilities of individuals in understanding healthy mental functioning together with mental disorders. This approach has been considered the most optimal for promoting well-being and decreasing the burden of diseases by cultivating habits, goals, and values in order to facilitate awareness about nurturing well-being. In line with this, personality development, mental growth, and escalation of self-awareness have been introduced” as the path to well-being. However, personality immaturity and low self-awareness have been strongly related to personality and mental disorders.32,33 The quantitative measure for personality development in this model is the mathematical summation of scores of character dimensions; however, five hierarchical levels of awareness (awarenesses of being, free will, beauty, truth, and goodness, respectively) and four states of self-awareness (unaware, average adult cognition, metacognition, and contemplation, respectively) have been theoretically defined in this model. Thereupon, details of temperament and character are widely used for person-centered neuro-pharmacological and psychosocial remedies.33 OCD treatment encounters various challenges, both in pharmacology and psychotherapy. Assessing the details of temperament and character could inaugurate clinical solutions in this regard.
To the best of our knowledge, no investigation has reported differences in character subscales in OCD. Therefore, the aim of the current study was to determine the temperament and character profile of OCD patients, including subscales and personality development. The researchers of the current study hypothesize that there is a profound and delicate interpersonal difficulty in OCD patients, apparent in their personality profile, which could guide toward more optimized psychobiologic treatments.
Methods
Subjects
Fifty-one patients, with a mean age of 30.59 ± 9.49, newly diagnosed OCD patients seeking professional care who had received no psychiatric treatment, were recruited from the Bozorgmehr Clinic (Psychology, Psychiatry, and Neurosciences Clinic) in Tabriz, Iran. An expert psychiatrist determined the diagnosis based on DSM-IV criteria for OCD assessed by the Structured Clinical Interview for DSM-IV (SCID).34 The patients were excluded from the study if they suffered from bipolar mood disorder, psychotic features, or substance abuse.
This investigation is a cross-sectional case-control study. As the control group, 53 subjects were recruited, with a mean age of 30.23 ± 9.41, who were unrelated to patients, free of psychiatric diseases, and enrolled from a sample of academic volunteers and their relatives. All patients and control subjects were Iranians, and most of them were Azeri.
Measurements
Dimensional personality scales and subscales were measured by the Temperament and Character Inventory (TCI-125),35 and the Persian (Farsi) version, which showed proper validity and reliability.36-38 This inventory includes 125 yes/no items that could identify seven factors of temperament and character and 3–5 subscales for each of them. Factors of temperament are named novelty seeking (NS), harm avoidance, reward dependence, and persistence (Table 1). The factors of character are self-directedness, cooperativeness, and self-transcendence. The subscales of these factors are presented in Tables 2, 3, and 4. According to the definitions of Cloninger, personality development occurs in character and is defined as the increase in the three-character dimensions. Personality development was calculated as the mathematical summation of scores in the three-character dimension.
Table 1.
DemographicCharacteristics of Obsessive-compulsive Disorder Patients and Healthy Controls
|
Demographics
|
Subjects
|
P
Value
|
|
OCD Patients
|
Healthy Controls
|
Total
|
| Age |
30.59 ± 9.49 |
30.23 ± 9.40 |
30.40 ± 9.40 |
0.85 |
| Male-female |
31.4-68.6%
(n = 16-35) |
30.2-69.8%
(n = 16-37) |
30.8-69.2%
(n = 32-72) |
0.90 |
| Single-married |
39.2-60.8%
(n = 20-31) |
39.6-60.4%
(n = 21-32) |
39.4-60.6%
(n = 41-63) |
0.96 |
| Ethnicity |
> 90%
Azeri, Iranian |
> 90%
Azeri, Iranian |
> 90%
Azeri, Iranian |
- |
| Education (years) |
14.53 ± 2.25 |
14.58 ± 4.31 |
14.56 ± 3.81 |
0.94 |
| Y-BOCS score |
20.55 ± 8.49 |
- |
- |
- |
Note. OCD: Obsessive-compulsive disorder; Y-BOCS: Yale-Brown Obsessive-Compulsive Scale.
Table 2.
Comparison of Temperament and Character Dimensions in Obsessive-Compulsive Disorder and Controls
|
Personality Dimensions
|
Subjects
|
P
Value
|
|
OCD Patients
|
Healthy Controls
|
|
Mean±SD
|
Range
|
Mean±SD
|
Range
|
| Temperament |
|
|
|
|
|
| Harm avoidance |
14.04 ± 3.65 |
3-19 |
9.36 ± 5.03 |
1-18 |
0.000a |
| Novelty seeking |
9.18 ± 4.39 |
1-17 |
8.17 ± 3.31 |
2-19 |
0.189 |
| Reward dependence |
8.49 ± 2.83 |
1-15 |
9.49 ± 2.39 |
9-14 |
0.054b |
| Persistence |
3.43 ± 1.58 |
0-5 |
2.60 ± 1.56 |
0-5 |
0.008a` |
| Character |
|
|
|
|
|
| Self-directedness |
9.37 ± 5.24 |
1-23 |
16.38 ± 4.68 |
6-24 |
0.000a |
| Cooperativeness |
15.88 ± 3.93 |
8-24 |
18.96 ± 4.76 |
2-25 |
0.001a |
| Self-transcendence |
8.14 ± 3.30 |
1-15 |
9.02 ± 3.94 |
1-15 |
0.220 |
| Personality development |
33.39 ± 8.13 |
13-54 |
44.36 ± 9.64 |
15-61 |
0.000a |
Note. OCD: Obsessive-compulsive disorder; SD: Standard deviation.
a
P < 0.01; b < 0.1 & > 0.05 (marginal significance).
Table 3.
Comparison of Temperament Subscales in Obsessive-compulsive Disorder and Controls
Personality
Lower Order Traits
|
Subjects
|
P
Value
|
|
OCD Patients
|
Healthy Controls
|
|
Mean±SD
|
Range
|
Mean±SD
|
Range
|
| Harm avoidance |
|
|
|
|
|
| Anticipatory worry |
3.08 ± 1.04 |
0-4 |
2.17 ± 1.16 |
0-4 |
0.000a |
| Fear of uncertainty |
4.65 ± 1.57 |
0-6 |
2.98 ± 2.06 |
0-6 |
0.000a |
| Shyness |
2.73 ± 1.59 |
0-5 |
1.91 ± 1.61 |
0-5 |
0.010a |
| Fatigability |
3.59 ± 0.75 |
1-5 |
2.30 ± 1.55 |
0-5 |
0.000a |
| Novelty seeking |
|
|
|
|
|
| Exploratory excitability |
2.71 ± 1.27 |
1-5 |
2.58 ± 1.17 |
0-5 |
0.614 |
| Impulsiveness |
2.20 ± 1.61 |
0-5 |
1.64 ± 1.47 |
0-5 |
0.069b |
| Extravagance |
2.18 ± 1.69 |
0-5 |
2.23 ± 1.53 |
0-5 |
0.875 |
| Disorderliness |
2.10 ± 1.30 |
0-5 |
1.72 ± 0.95 |
0-4 |
0.090b |
| Reward dependence |
|
|
|
|
|
| Sentimentality |
3.65 ± 1.13 |
1-5 |
3.60 ± 1.18 |
1-5 |
0.849 |
| Attachment |
2.43 ± 1.72 |
0-5 |
3.19 ± 1.39 |
0-5 |
0.015c |
| Dependence |
2.57 ± 1.19 |
1-5 |
2.70 ± 1.27 |
0-5 |
0.592 |
Note. OCD: Obsessive-compulsive disorder; SD: Standard deviation.
a P < 0.01; b < 0.1 & > 0.05 (marginal significance); cP < 0.05.
Table 4.
Comparison of Character Subscales in Obsessive-compulsive Disorder and Controls
Personality
Lower Order Traits
|
Subjects
|
P
Value
|
|
OCD Patients
|
Healthy Controls
|
|
|
Mean±SD
|
Range
|
Mean±SD
|
Range
|
| Self-directedness |
|
|
|
|
|
| Responsibility |
1.86 ± 1.40 |
0-5 |
3.47 ± 1.44 |
0-5 |
0.000a |
| Purposeful |
1.92 ± 1.43 |
0-5 |
3.87 ± 1.23 |
1-5 |
0.000a |
| Resourcefulness |
2.22 ± 1.50 |
0-5 |
3.94 ± 1.28 |
1-5 |
0.000a |
| Self-acceptance |
1.63 ± 1.48 |
0-5 |
2.17 ± 1.55 |
0-5 |
0.072b |
| Enlightened second nature (spontaneity) |
1.78 ± 1.45 |
0-5 |
2.92 ± 1.45 |
0-5 |
0.000a |
| Cooperativeness |
|
|
|
|
|
| Social acceptance (tolerance) |
2.69 ± 1.36 |
0-5 |
3.74 ± 1.44 |
0-5 |
0.000a |
| Empathy |
3.39 ± 1.02 |
1-5 |
3.45 ± 1.22 |
0-5 |
0.784 |
| Helpfulness |
3.29 ± 1.05 |
1-5 |
3.68 ± 1.25 |
0-5 |
0.092b |
| Compassion |
2.96 ± 1.54 |
0-5 |
3.87 ± 1.24 |
0-5 |
0.000a |
| Pure-hearted conscience (principledness) |
3.55 ± 0.99 |
2-5 |
4.23 ± 1.07 |
0-5 |
0.000a |
| Self-transcendence |
|
|
|
|
|
| Spiritual acceptance |
3.43 ± 1.56 |
0-5 |
3.53 ± 1.76 |
1-5 |
0.768 |
| Self-forgetfulness |
2.25 ± 1.40 |
0-5 |
2.36 ± 1.56 |
0-5 |
0.722 |
| Transpersonal identification |
2.45 ± 1.24 |
0-5 |
3.13 ± 1.37 |
0-5 |
0.009a |
Note. OCD: Obsessive-compulsive disorder; SD: Standard deviation.
a P < 0.01; b < 0.1 & > 0.05 (marginal significance).
The severity of OCD was assessed by the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS), which includes ten items about the presence of symptoms and distress, with scores ranging from zero (not at all) to 4 (extreme and disability).39
Statistical Analysis
Descriptive analyses were performed. The internal consistency of the questionnaires used in this study was assessed, including Cronbach’s alpha coefficients for Y-BOCS, for TCI for temperament calculations, and for character calculations. The correlation between forms, the Spearman-Brown coefficient, and the Guttman Split-Half coefficient was assessed as well.
The distribution of the investigated variables was analyzed using the one-sample Kolmogorov-Smirnov test, where an insignificant difference implies a normal distribution (P= 0.05).
The difference in the scores of scales and subscales in the TCI of patients and controls was analyzed by multiple analyses of variance in order to correct errors regarding multiple analyses. Box’s test of equality of covariance matrices and the Hetling effect were incorporated. In this analysis, an item, including several variables, is compared in cases and controls, and then a variable-by-variable comparison is made. The overall comparison by Box’s test of equality of covariance matrices shows uniformity between the two groups if there is no significant difference in this test, for which the significance level is 0.23. Then, a variable-by-variable comparison is made using the Hetling effect and considering the F value and P value (0.05), and thereupon statistical significance is demonstrated.
Logistic regression analysis was performed for temperament and character factors in the two groups in order to propose factors that could predict OCD affliction. Moreover, Pearson correlation analysis was conducted for temperament and character scales and subscales, and OCD severity.
The Statistical Package of the Social Sciences (SPSS) software was used, and significance was considered as P values less than 0.05.
Results
The characteristics of patients and controls with regard to demographic parameters and OCD severity are summarized in Table 1.
Internal consistency estimates were Cronbach’s alpha of 0.89 for Y-BOCS, and Cronbach’s alpha coefficients of 0.76 and 0.74 for TCI for the temperament and character calculations, respectively. The correlation between forms was 0.71, and the Spearman-Brown and Guttman Split-Half coefficients were both 0.83.
The investigated variables demonstrated a normal distribution (P > 0.05),except for harm avoidance (P = 0.02) and persistence (P = 0.00).
Several temperament and character factors showed significant differences in the two groups, with OCD patients representing a highly significant increase in harm avoidance and persistence, as well as marginally lower reward dependence, in the temperament, while there was a highly significant decrease in self-directedness and cooperativeness in the character. The mean scores of seven personality factors and their statistical differences in OCD patients and control subjects are summarized in Table 2.
The analyses of subscales revealed statistical differences for numerous traits, both in factors that showed significant differences and those that did not. The mean scores of the 25 subscales and their statistical differences are provided in Tables 3 and 4. OCD patients demonstrated highly significant increases in anticipatory worry, fear of uncertainty, shyness, and fatigability. Conversely, they showed highly significant decreases in attachment, responsibility, purposefulness, resourcefulness, spontaneity, tolerance, compassion, principledness, and transpersonal identification.
Logistic regression analysis indicated no significant values for NS, harm avoidance, or cooperativeness for predicting OCD affliction (P = 0.24-0.88). However, the persistence (P = 0.01) and self-directedness (P = 0.00) scores could positively and negatively predict OCD affliction, respectively. Marginal trends existed toward reward dependence (P = 0.05) and self-transcendence (P = 0.06), negatively predicting OCD affliction.
Figure 1 illustrates the distribution of OCD severity in patients.
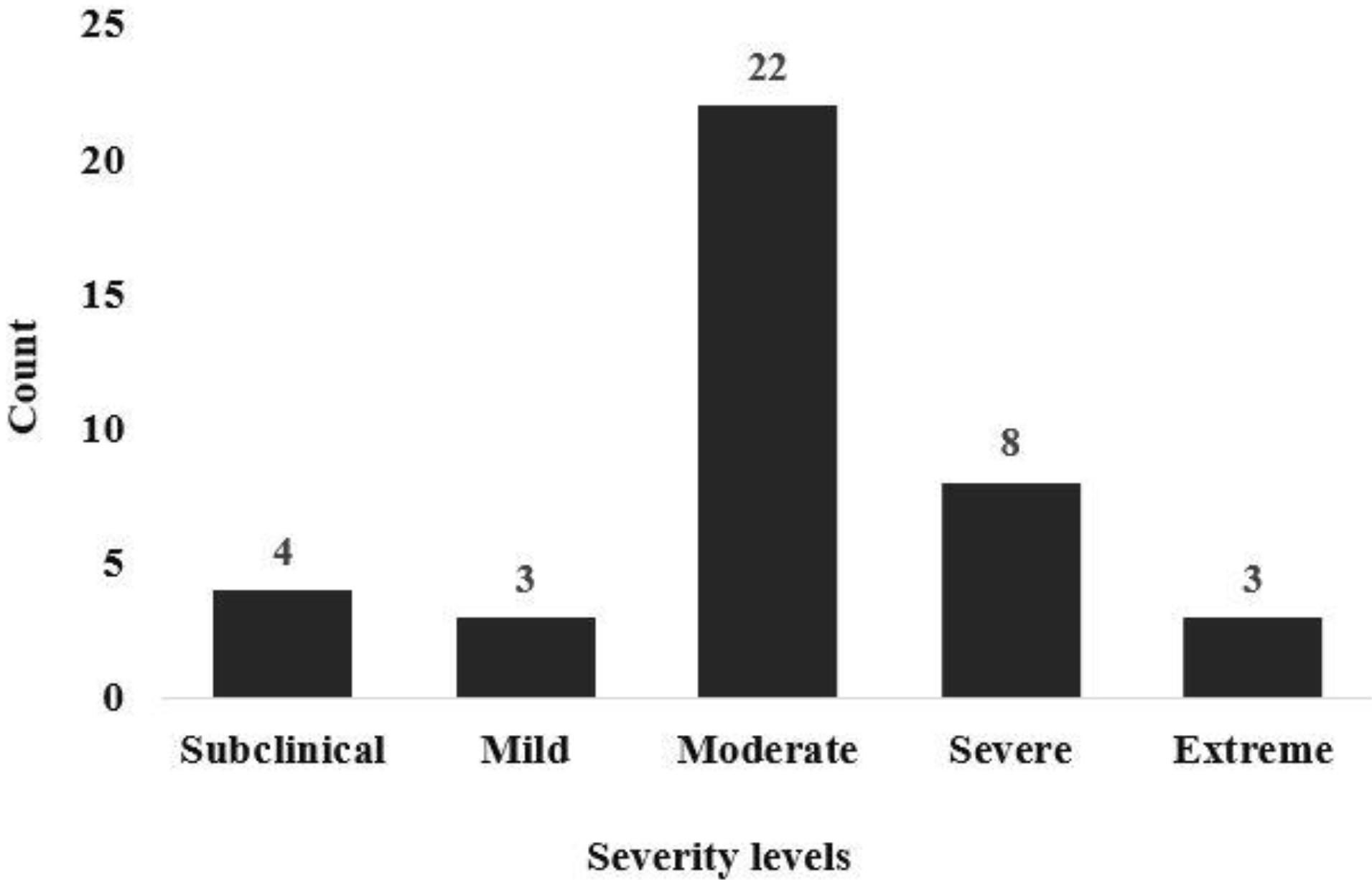
Figure 1.
Number of Patients With OCD of Various Severity Levels. Note. OCD: Obsessive-compulsive disorder
.
Number of Patients With OCD of Various Severity Levels. Note. OCD: Obsessive-compulsive disorder
Pearson correlation between TCI scales and subscales and OCD severity revealed no significant values (P = 0.11-0.98); however, marginal significance was shown for persistence (P = 0.06) and the attachment subscale of reward dependence (P = 0.08).
Discussion
A detailed profile of temperament and character in OCD patients was evaluated in the current study, demonstrating significant differences in the factors and lower traits of nearly most of the dimensions of temperament and character, bearing more significance in harm avoidance, persistence, self-directedness, cooperativeness, and outstanding personality development. To the best of our knowledge, there is no previous report about subscales (lower-order traits or component facets) of character dimensions in OCD patients.
An integrative view of changes in temperament and lower-order character traits could lead to the conclusion that OCD lies in interpersonal personality difficulties. The findings of the current investigation demonstrated that OCD patients have higher shyness, lower attachment, lower tolerance, lower compassion, lower principledness, and lower transpersonal identification, all of which highlight interpersonal difficulties in various temperament and character factors.
An outstanding characteristic of temperament and the character model of personality is its unique capability to guide toward pharmacotherapies and psychotherapies. Psychotherapies in this regard focusing on mental growth, level of self-awareness, psychodynamic formulations, and relation with categorical personality disorders are in deep involvement with subscales; hence, investigating the seven-factor subscales, together with personality development leading to an appropriate discussion, could be considered an acceptable novelty for the current study.
The psychobiological personality model proposed by Cloninger was initiated by the introduction of the tridimensional model determining temperament as the biogenetic domain of personality. This domain implies mental processing, which is innate and procedural with an independent heritage, specifically related to neurotransmitter systems and, therefore, to some of the pharmacotherapies. Dimensions of this domain included harm avoidance, NS, and reward dependence, and subsequently, the dimension of persistence was added to them. The dimension of harm avoidance was demonstrated to be highly different in OCD patients in the most classic studies in this regard26,28 and all the following studies.19-21,23,25,27,29,40-42 Richter et al reported a correlation between harm avoidance and all of its subscales (i.e., anticipatory worry, fear of uncertainty, shyness, and fatigability),30 which conforms to our findings, demonstrating a highly significant increase in harm avoidance and its subscales (i.e., anticipatory worry, fear of uncertainty, shyness, and fatigability; P= 0.00). This infers an inborn tendency toward evading any negative consequence, which is strongly true in all the lower domains of harm avoidance. This concept was further reinforced by the previous research about Gray’s theory of personality about the Behavioral Inhibitions System (BIS) and Behavioral Activation System (BAS), which showed significant increases in BIS (i.e., higher sensitivity to punishment).17,18 The textbook of Psychiatry32 “proposes a stepwise path of character development to well-being, and emphasis is placed on the reconciliation of emotional conflicts that can be measured by the extremes of each of the temperament dimensions; these extremes are transcended by spiritually elevated thoughts. For example, self-respect reconciles the extremes of harm avoidance”. Moreover, the high shyness subscale could be modulated by increased interpersonal skills. Nevertheless, harm avoidance is closely related to the serotonin neurotransmitter system in the brain, and thereby, serotonergic pharmacologic agents control some symptoms in the short term and decrease harm avoidance in the long term. The standard treatment of OCD with selective-serotonin reuptake inhibitors (SSRIs) has proved a significant decrease in the harm avoidance factor, though not returning it to levels similar to healthy controls, as well as a significant increase in reward dependence, though not deviating from healthy controls.19,27,29,40 This modulation could be considered contributory to the SSRI remedy in OCD, and it emphasizes the importance of the temperament profile in this disorder. Generally, personality backgrounds have proven to be influential in the psychotherapy of anxiety disorders.42
The relationship between other temperament elements and OCD has appeared inconsistent in the literature. Based on the findings of the current study, marginally significant decreases were observed in reward dependence and the attachment subscale of reward dependence in OCD patients. While most studies have reported no significant difference or correlation for reward dependence, one investigation found lower scores for reward dependence in OCD patients.23 Contrarily, the results of the classic study by Pfohl et al26 showed higher scores for reward dependence. The main findings of both the previous studies and the present study indicate that attention to reward and interpersonal clues might be related to OCD in particular domains. As mentioned above, there are multiple personality difficulties in various lower-order personality traits in OCD patients. These patients might not seem highly different in sentimentality or dependence, but they may seem rather cold, experiencing deep attachments less than others. Thus, activating the noradrenergic neurotransmittering system in the median raphe both by pharmacologic agents or psychotherapies aimed at interpersonal experiences may alleviate some of the OCD presentations. Moreover, SSRI pharmacotherapies could pose some beneficence, as mentioned earlier.
Similarly, NS is reported unchanged in most studies; however, Alonso et al and Kusunoki et al reported lower scores of NS.19,43 Some Iranian studies have shown significant differences or correlations for NS in OCD patients toward lower scores.44 The dimension of NS presented unchanged in the current investigation; nevertheless, the subscales of impulsiveness and disorderliness demonstrated marginally significant increases (P =0.049). Other subscales of NS were displayed as statistically similar. This is apparently opposite to the findings of Fullana et al17,18; they utilized the Sensitivity to Punishment and Sensitivity to Reward Questionnaire and reported low impulsivity in OCD patients with hoarding symptoms. Nonetheless, it should be noted that “impulse” is considered a dimension of OCD symptoms. Moreover, impulsivity is related to psychotism in the PEN model in Eysenck’s theory, but this dimension was not proven to be related to OCD.14 A recent study has revealed that OCD-compulsive rituals might be directed by a negative reinforcing network, similar to drug addiction but different from the two major components of addiction, which are risky decision-making and behavioral impulsivity.45 Overall, innate reactions about novelty and diversity with all the subscales of exploration, impulsivity, extravagance, and disorderliness could be considered as having no or weak relations with OCD. However, they could be specified for those OCD patients who may show higher impulsivity character goals of self-mastery and impulse control, and psychoeducation about self-efficacy, biorhythms, nutrition, and impulsivity reconciliation could be efficient.32
The dimension of persistence, which has been introduced as a relatively intermediate factor on the border of the two temperament and character domains, was demonstrated to be higher in OCD patients in the current study. However, most studies confirmed that it was unaffected, except for a few studies that indicated even lower scores.22 Kim et al reported that higher persistence was a predictor of a higher scale on the hoarding dimension.23
Character is the domain of the personality model of Cloninger, which points to the acquired traits and concepts of the individual about self, others, and the world. The advent of personality development and maturity in character brings about the meaning of inner growth and mental escalation, which is actually increasing the scores of character dimensions.33 The first dimension of character, self-directedness, has proven to be significantly decreased in OCD patients.19,22,23,25,29,40,42,43 Self-directedness has also been correlated with OCD severity.22,29 However, other studies did not find such a correlation.19,40 This implies that lower responsibility, purposefulness, resourcefulness, and enlightened second nature are common in OCD patients. Interestingly, treatment with SSRIs, which modulated the temperament, did not alter self-directedness.29,40 This establishes the influential position of psychotherapies for the treatment of OCD, especially if they focus on personality development rather than necessarily focusing on OCD symptoms. Moreover, the obtained results imply actually a relatively higher level of self-acceptance when all other subscales of self-directedness are taken into consideration.
These findings may contradict the idea that an increased sense of responsibility is a key symptom in many OCD patients. According to Kaplan and Sadock’s Comprehensive Textbook Psychiatry,32 “character refers to the mind, that is, the conceptual core of personality, which reflects personal goals and values; what individuals make of themselves intentionally. Character is rational and volitional, described as one’s mental self-government. Character traits are adaptive, and their low ends, personality immaturity, are less adaptive. Self-directedness and its subscales quantify executive competence, and a highly self-directed person is self-sufficient, realistic, effective, and highly adaptive.” OCD patients demonstrate maladaptive perfectionism or obsessive involvement with various affairs or duties.46 Samuels et al have reported relations between conscientiousness and OCPD.47 However, these characteristics differ from responsibility, defined as a subscale of self-directedness.
There are also consistent results about decreased cooperativeness. In line with the results of many studies,19,20,22,23,42,43 our findings indicated a significant decrease in cooperativeness while adding a significant decrease in three of its subscales, namely, social acceptance, compassion, and pure-hearted conscience. These results point out the fact that maturity in interpersonal and social relationships might alleviate OCD affliction. To alleviate these personality defects in OCD patients, the character goals of secure human attachments and approval-seeking reconciliation could be efficient.32
Moreover, the mentioned decreased subscales of self-directedness and cooperativeness imply the important fact that the self-awareness of OCD patients is diminished even in the lower levels of awareness of being and awareness of free will, and this should be in mind in psychotherapies, psychodynamic formulations, and transcendental approaches.
Self-transcendence has rarely been mentioned in the personality profiles of OCD patients; Karimi Yousefi et al reported highly significant decreases in self-transcendence in high school female students with OCD. In the current investigation, the dimension of self-transcendence showed no significant difference, while the subscale of transpersonal identification was significantly decreased. Nevertheless, the combination of higher self-transcendence and lower self-directedness has been reported to be correlated with the symmetry/ordering and sexual/religious dimensions of OCD.23 The combination of higher self-transcendence, lower self-directedness, and cooperativeness is introduced as the fanatic personality type in Cloninger’s model.31,33,48 Overall, the scores of character dimensions manifest the fact that a balanced personality development through the concordant increase of all character dimensions could induce mental normality against the personality profile in OCD. The score of personality development as the sum of scores of the three-character dimensions was decreased with high significance in the OCD patients of the present study. Consequently, the hierarchical levels of awareness proposed by Cloninger33 are diminished in OCD patients at nearly all levels. Levels of awareness for mental escalation in the Cloninger’s model incorporate each of the consecutive subscales of self-directedness, cooperativeness, and self-transcendence as one of the levels of awareness, and this could be considered in the OCD-related personality profile of subscales obtained in this study, especially for beneficial psychotherapy for these patients.
Some limitations ought to be mentioned, along with the outcomes of the current study. The obtained results could be more precise if the depression and anxiety of the subjects and other variables, such as illness duration, were evaluated, and the results were justified accordingly. Moreover, the control sample has been selected from an academic sample and their relatives, while the patients have been selected from a clinic. Although age, gender, marital status, and ultimately the educational years of patients and controls were matched, the detailed socioeconomic levels of the two groups may have been different.
Conclusion
Significant differencesin the scores of the TCI seven factors and subscales in OCD patients were demonstrated toward higher harm avoidance, lower self-directedness, and cooperativeness. The profile of subscales showed higher anticipatory worry, fear of uncertainty, shyness, and fatigability, along with lower responsibility, purposefulness, resourcefulness, enlightened second nature, social acceptance, compassion, pure-hearted conscience, and transpersonal identification. This profile could be incorporated for further comprehension of OCD and more specific pharmacotherapies and psychotherapies. Psychotherapies are suggested to focus on personality development by increasing character subscales rather than merely on OCD symptoms.
Acknowledgements
This study was part of two MD theses, which supported by the Research Center of Psychiatry and Behavioral Sciences at Tabriz University of Medical Sciences, Tabriz, Iran (Grant number: 009599). We wish to sincerely thank the patients and colleagues who participated in this study.
Authors’ Contribution
Conceptualization: Masumeh Zamanlu.
Data curation: Amirreza Azarmnia.
Formal analysis: Afra Pirahmadi.
Funding acquisition: Alireza Farnam.
Investigation: Masumeh Zamanlu.
Methodology: Alireza Farnam.
Resources: Alireza Farnam.
Software: Amirreza Azarmnia.
Supervision: Masumeh Zamanlu.
Validation: Afra Pirahmadi.
Visualization: Amirreza Azarmnia.
Writing–original draft: Afra Pirahmadi.
Writing–review & editing: Masumeh Zamanlu.
Competing Interests
None.
Ethical Approval
The current study has been approved by the Ethics Committee of Tabriz University of Medical Sciences (Codes: IR.TBZMED.REC.1396.988 and IR.TBZMED.REC.1396.989), and patients and controls signed an informed consent form before incorporation.
Funding
None.
References
- Stein DJ. Obsessive-compulsive disorder. Lancet 2002; 360(9330):397-405. doi: 10.1016/s0140-6736(02)09620-4 [Crossref] [ Google Scholar]
- Steinberger K, Schuch B. Classification of obsessive-compulsive disorder in childhood and adolescence. Acta Psychiatr Scand 2002; 106(2):97-102. doi: 10.1034/j.1600-0447.2002.02220.x [Crossref] [ Google Scholar]
- Storch EA, Abramowitz J, Goodman WK. Where does obsessive-compulsive disorder belong in DSM-V?. Depress Anxiety 2008; 25(4):336-47. doi: 10.1002/da.20488 [Crossref] [ Google Scholar]
- Leckman JF, Denys D, Simpson HB, Mataix-Cols D, Hollander E, Saxena S. Obsessive-compulsive disorder: a review of the diagnostic criteria and possible subtypes and dimensional specifiers for DSM-V. Depress Anxiety 2010; 27(6):507-27. doi: 10.1002/da.20669 [Crossref] [ Google Scholar]
- Leckman JF, Zhang H, Alsobrook JP, Pauls DL. Symptom dimensions in obsessive-compulsive disorder: toward quantitative phenotypes. Am J Med Genet 2001; 105(1):28-30. [ Google Scholar]
- Rachman S, de Silva P. Abnormal and normal obsessions. Behav Res Ther 1978; 16(4):233-48. doi: 10.1016/0005-7967(78)90022-0 [Crossref] [ Google Scholar]
- Salkovskis PM. Obsessional-compulsive problems: a cognitive-behavioural analysis. Behav Res Ther 1985; 23(5):571-83. doi: 10.1016/0005-7967(85)90105-6 [Crossref] [ Google Scholar]
- Muris P, Merckelbach H, Clavan M. Abnormal and normal compulsions. Behav Res Ther 1997; 35(3):249-52. doi: 10.1016/s0005-7967(96)00114-3 [Crossref] [ Google Scholar]
- Phillips KA, Stein DJ, Rauch SL, Hollander E, Fallon BA, Barsky A. Should an obsessive-compulsive spectrum grouping of disorders be included in DSM-V?. Depress Anxiety 2010; 27(6):528-55. doi: 10.1002/da.20705 [Crossref] [ Google Scholar]
- Baer L. Factor analysis of symptom subtypes of obsessive-compulsive disorder and their relation to personality and tic disorders. J Clin Psychiatry 1994; 55 Suppl:18-23. [ Google Scholar]
- Gordon OM, Salkovskis PM, Bream V. The impact of obsessive-compulsive personality disorder on cognitive behaviour therapy for obsessive-compulsive disorder. Behav Cogn Psychother 2016; 44(4):444-59. doi: 10.1017/s1352465815000582 [Crossref] [ Google Scholar]
- Joffe RT, Swinson RP, Regan JJ. Personality features of obsessive-compulsive disorder. Am J Psychiatry 1988; 145(9):1127-9. doi: 10.1176/ajp.145.9.1127 [Crossref] [ Google Scholar]
- Sadri SK, McEvoy PM, Egan SJ, Kane RT, Rees CS, Anderson RA. The relationship between obsessive-compulsive personality and obsessive-compulsive disorder treatment outcomes: predictive utility and clinically significant change. Behav Cogn Psychother 2017; 45(5):524-9. doi: 10.1017/s1352465817000194 [Crossref] [ Google Scholar]
- Scarrabelotti MB, Duck JM, Dickerson MM. Individual differences in obsessive-compulsive behaviour: the role of the Eysenckian dimensions and appraisals of responsibility. Pers Individ Dif 1995; 18(3):413-21. doi: 10.1016/0191-8869(94)00122-9 [Crossref] [ Google Scholar]
- Samuels J, Nestadt G, Bienvenu OJ, Costa PT Jr, Riddle MA, Liang KY. Personality disorders and normal personality dimensions in obsessive-compulsive disorder. Br J Psychiatry 2000; 177:457-62. doi: 10.1192/bjp.177.5.457 [Crossref] [ Google Scholar]
- Summerfeldt LJ, Huta V, Swinson RP. Personality and obsessive-compulsive disorder. In: Obsessive-Compulsive Disorder: Theory, Research, and Treatment. Guilford Press; 1998. p. 79-119.
- Fullana MA, Mataix-Cols D, Caseras X, Alonso P, Manuel Menchón J, Vallejo J. High sensitivity to punishment and low impulsivity in obsessive-compulsive patients with hoarding symptoms. Psychiatry Res 2004; 129(1):21-7. doi: 10.1016/j.psychres.2004.02.017 [Crossref] [ Google Scholar]
- Fullana MA, Mataix-Cols D, Trujillo JL, Caseras X, Serrano F, Alonso P. Personality characteristics in obsessive-compulsive disorder and individuals with subclinical obsessive-compulsive problems. Br J Clin Psychol 2004; 43(Pt 4):387-98. doi: 10.1348/0144665042388937 [Crossref] [ Google Scholar]
- Alonso P, Menchón JM, Jiménez S, Segalàs J, Mataix-Cols D, Jaurrieta N. Personality dimensions in obsessive-compulsive disorder: relation to clinical variables. Psychiatry Res 2008; 157(1-3):159-68. doi: 10.1016/j.psychres.2006.06.003 [Crossref] [ Google Scholar]
- Bejerot S, von Knorring L, Ekselius L. Personality traits and smoking in patients with obsessive-compulsive disorder. Eur Psychiatry 2000; 15(7):395-401. doi: 10.1016/s0924-9338(00)00509-5 [Crossref] [ Google Scholar]
- Bey K, Lennertz L, Riesel A, Klawohn J, Kaufmann C, Heinzel S. Harm avoidance and childhood adversities in patients with obsessive-compulsive disorder and their unaffected first-degree relatives. Acta Psychiatr Scand 2017; 135(4):328-38. doi: 10.1111/acps.12707 [Crossref] [ Google Scholar]
- Cruz-Fuentes C, Blas C, Gonzalez L, Camarena B, Nicolini H. Severity of obsessive-compulsive symptoms is related to self-directedness character trait in obsessive-compulsive disorder. CNS Spectr 2004; 9(8):607-12. doi: 10.1017/s1092852900002789 [Crossref] [ Google Scholar]
- Kim SJ, Kang JI, Kim CH. Temperament and character in subjects with obsessive-compulsive disorder. Compr Psychiatry 2009; 50(6):567-72. doi: 10.1016/j.comppsych.2008.11.009 [Crossref] [ Google Scholar]
- Kim SW, Grant JE. Personality dimensions in pathological gambling disorder and obsessive-compulsive disorder. Psychiatry Res 2001; 104(3):205-12. doi: 10.1016/s0165-1781(01)00327-4 [Crossref] [ Google Scholar]
- Lyoo IK, Lee DW, Kim YS, Kong SW, Kwon JS. Patterns of temperament and character in subjects with obsessive-compulsive disorder. J Clin Psychiatry 2001; 62(8):637-41. doi: 10.4088/jcp.v62n0811 [Crossref] [ Google Scholar]
- Pfohl B, Black D, Noyes R Jr, Kelley M, Blum N. A test of the tridimensional personality theory: association with diagnosis and platelet imipramine binding in obsessive-compulsive disorder. Biol Psychiatry 1990; 28(1):41-6. doi: 10.1016/0006-3223(90)90430-a [Crossref] [ Google Scholar]
- Ranjana T, Daya R, Srivastava M. Temperament and character profile in obsessive-compulsive disorder (OCD): a pre and post intervention analysis. Int J Sch Cogn Psychol 2014; 1(2):106. doi: 10.4172/2469-9837.1000106 [Crossref] [ Google Scholar]
- Richter J, Brändström S. Personality disorder diagnosis by means of the Temperament and Character Inventory. Compr Psychiatry 2009; 50(4):347-52. doi: 10.1016/j.comppsych.2008.09.002 [Crossref] [ Google Scholar]
- Albert U, De Ronchi D, Maina G, Pompili M. Suicide Risk in Obsessive-Compulsive Disorder and Exploration of Risk Factors: A Systematic Review. Curr Neuropharmacol 2019; 17(8):681-696. doi: 10.2174/1570159X16666180620155941 [Crossref] [ Google Scholar]
- Richter MA, Summerfeldt LJ, Joffe RT, Swinson RP. The Tridimensional Personality Questionnaire in obsessive-compulsive disorder. Psychiatry Res 1996; 65(3):185-8. doi: 10.1016/s0165-1781(96)02944-7 [Crossref] [ Google Scholar]
- Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Lippincott Williams & Wilkins; 2011.
- Sadock BJ, Sadock VA, Ruiz P. Kaplan and Sadock’s Comprehensive Textbook of Psychiatry. 10th ed. Wolters Kluwer; 2017.
- Cloninger CR. Feeling Good: The Science of Well-Being. Oxford University Press; 2004.
- Sharifi V, Assadi SM, Mohammadi MR, Amini H, Kaviani H, Semnani Y. a Persian translation of the structured clinical interview for diagnostic and statistical manual of mental disorders, fourth edition: psychometric properties. Compr Psychiatry 2009; 50(1):86-91. doi: 10.1016/j.comppsych.2008.04.004 [Crossref] [ Google Scholar]
- Cloninger CR, Przybeck TR, Svrakic DM, Wetzel RD. The Temperament and Character Inventory (TCI): A Guide to its Development and Use. St. Louis, Missouri: Washington University; 1994.
- Richter J, Brändström S, Emami H, Ghazinour M. An Iranian (Farsi) version of the Temperament and Character Inventory: a cross-cultural comparison. Psychol Rep 2007; 100(3 Pt 2):1218-28. doi: 10.2466/pr0.100.4.1218-1228 [Crossref] [ Google Scholar]
- Miettunen J, Kantojärvi L, Veijola J, Järvelin MR, Joukamaa M. International comparison of Cloninger’s temperament dimensions. Pers Individ Dif 2006; 41(8):1515-26. doi: 10.1016/j.paid.2006.06.006 [Crossref] [ Google Scholar]
- Dadfar M, Bahrami F, Dadfar F, Younesi SJ. Reliability and validity of the Temperament and Character Inventory. J Rehabil 2010; 11(3):15-24. [ Google Scholar]
- Kim SW, Dysken MW, Kuskowski M. The Yale-Brown obsessive-compulsive scale: a reliability and validity study. Psychiatry Res 1990; 34(1):99-106. doi: 10.1016/0165-1781(90)90061-9 [Crossref] [ Google Scholar]
- Lyoo IK, Yoon T, Kang DH, Kwon JS. Patterns of changes in Temperament and Character Inventory scales in subjects with obsessive-compulsive disorder following a 4-month treatment. Acta Psychiatr Scand 2003; 107(4):298-304. doi: 10.1034/j.1600-0447.2003.00054.x [Crossref] [ Google Scholar]
- Farnam A, Farhang S, Bakhshipour A, Niknam E. The five-factor model of personality in mixed anxiety-depressive disorder and effect on therapeutic response. Asian J Psychiatr 2011; 4(4):255-7. doi: 10.1016/j.ajp.2011.10.001 [Crossref] [ Google Scholar]
- Bejerot S, Schlette P, Ekselius L, Adolfsson R, von Knorring L. Personality disorders and relationship to personality dimensions measured by the Temperament and Character Inventory in patients with obsessive-compulsive disorder. Acta Psychiatr Scand 1998; 98(3):243-9. doi: 10.1111/j.1600-0447.1998.tb10075.x [Crossref] [ Google Scholar]
- Kusunoki K, Sato T, Taga C, Yoshida T, Komori K, Narita T. Low novelty-seeking differentiates obsessive-compulsive disorder from major depression. Acta Psychiatr Scand 2000; 101(5):403-5. doi: 10.1034/j.1600-0447.2000.101005403.x [Crossref] [ Google Scholar]
- Mohammadzadeh A, Rezaie A, Yaghoubi H, Pirkhaefi A. The relationship between obsessive compulsive and schizotypal personality features among university students. Iran J Psychiatry Clin Psychol 2011;16(4):490-5. [Persian].
- Abramovitch A, McKay D. Behavioral impulsivity in obsessive-compulsive disorder. J Behav Addict 2016; 5(3):395-7. doi: 10.1556/2006.5.2016.029 [Crossref] [ Google Scholar]
- Frost RO, Steketee G. Perfectionism in obsessive-compulsive disorder patients. Behav Res Ther 1997; 35(4):291-6. doi: 10.1016/s0005-7967(96)00108-8 [Crossref] [ Google Scholar]
- Samuels J, Bienvenu OJ, Krasnow J, Wang Y, Grados MA, Cullen B. An investigation of doubt in obsessive-compulsive disorder. Compr Psychiatry 2017; 75:117-24. doi: 10.1016/j.comppsych.2017.03.004 [Crossref] [ Google Scholar]
- Farmer RF, Goldberg LR. Brain modules, personality layers, planes of being, spiral structures, and the equally implausible distinction between TCI-R “temperament” and “character” scales: a reply to Cloninger. Psychol Assess 2008; 20(3):300-4. doi: 10.1037/a0012932 [Crossref] [ Google Scholar]